Email Alert | RSS 帮助

中国防痨杂志 ›› 2024, Vol. 46 ›› Issue (6): 687-698.doi: 10.19982/j.issn.1000-6621.20240127
李瑶, 方喆, 罗丹霖, 胡艳梅, 唐蜜, 唐志冈, 文新民, 张勇, 姚碧波, 王起, 易恒仲( )
)
Li Yao, Fang Zhe, Luo Danlin, Hu Yanmei, Tang Mi, Tang Zhigang, Wen Xinmin, Zhang Yong, Yao Bibo, Wang Qi, Yi Hengzhong()
摘要:
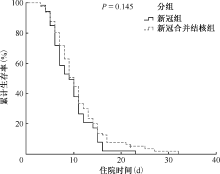
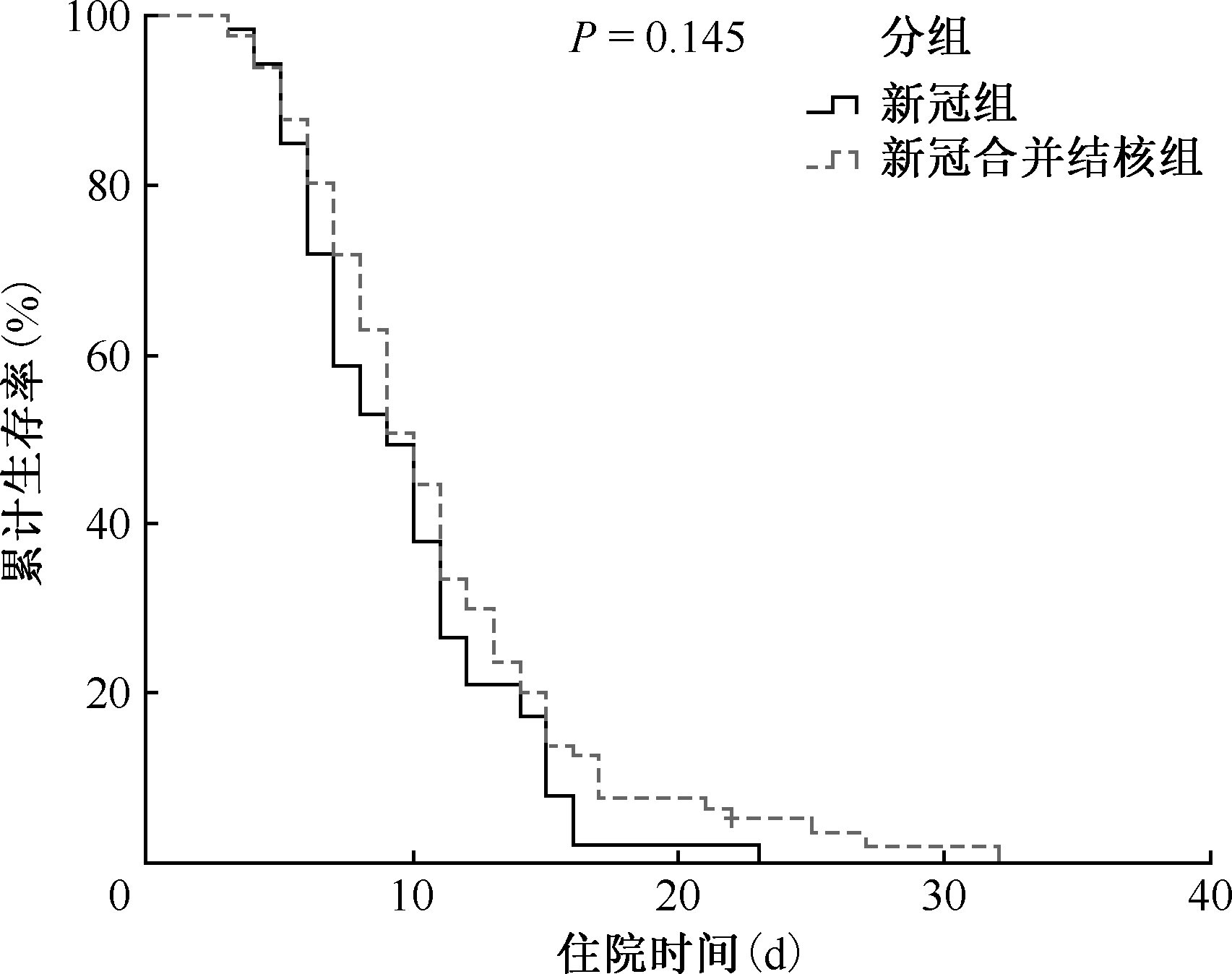
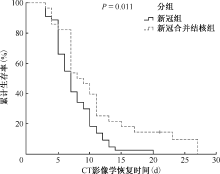
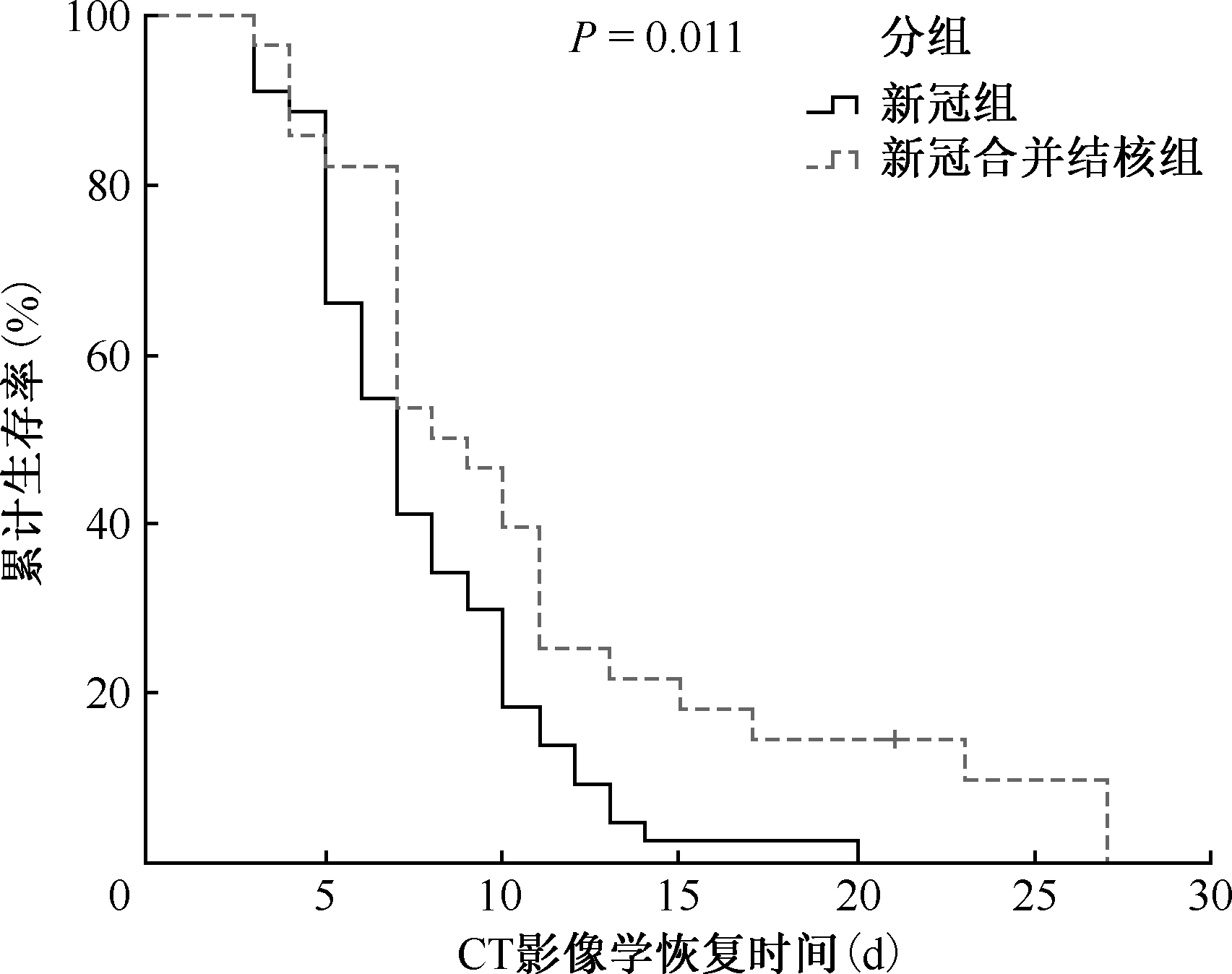
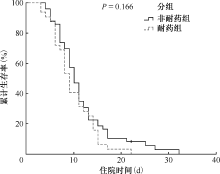
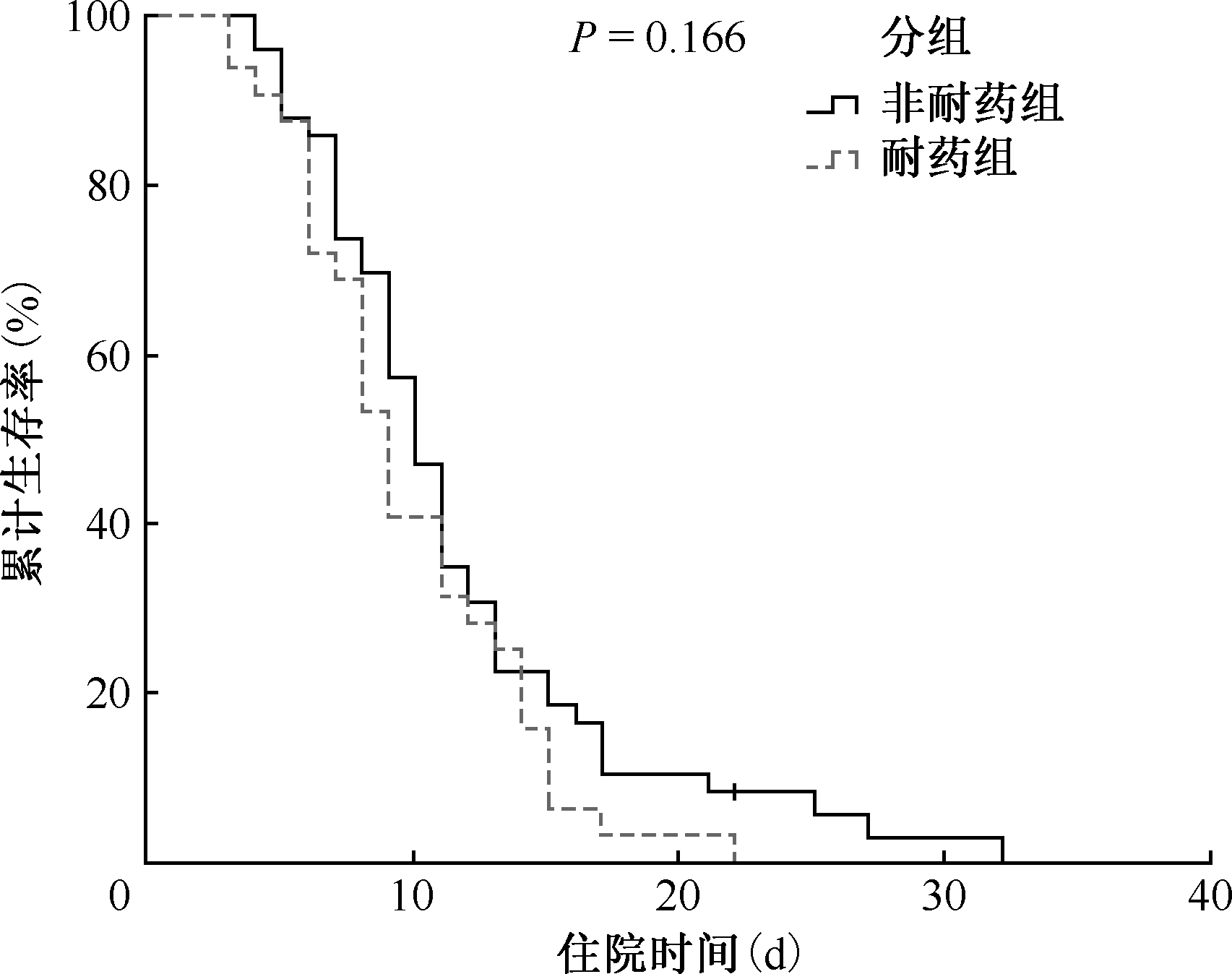
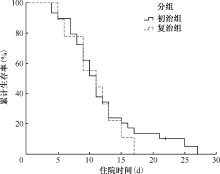
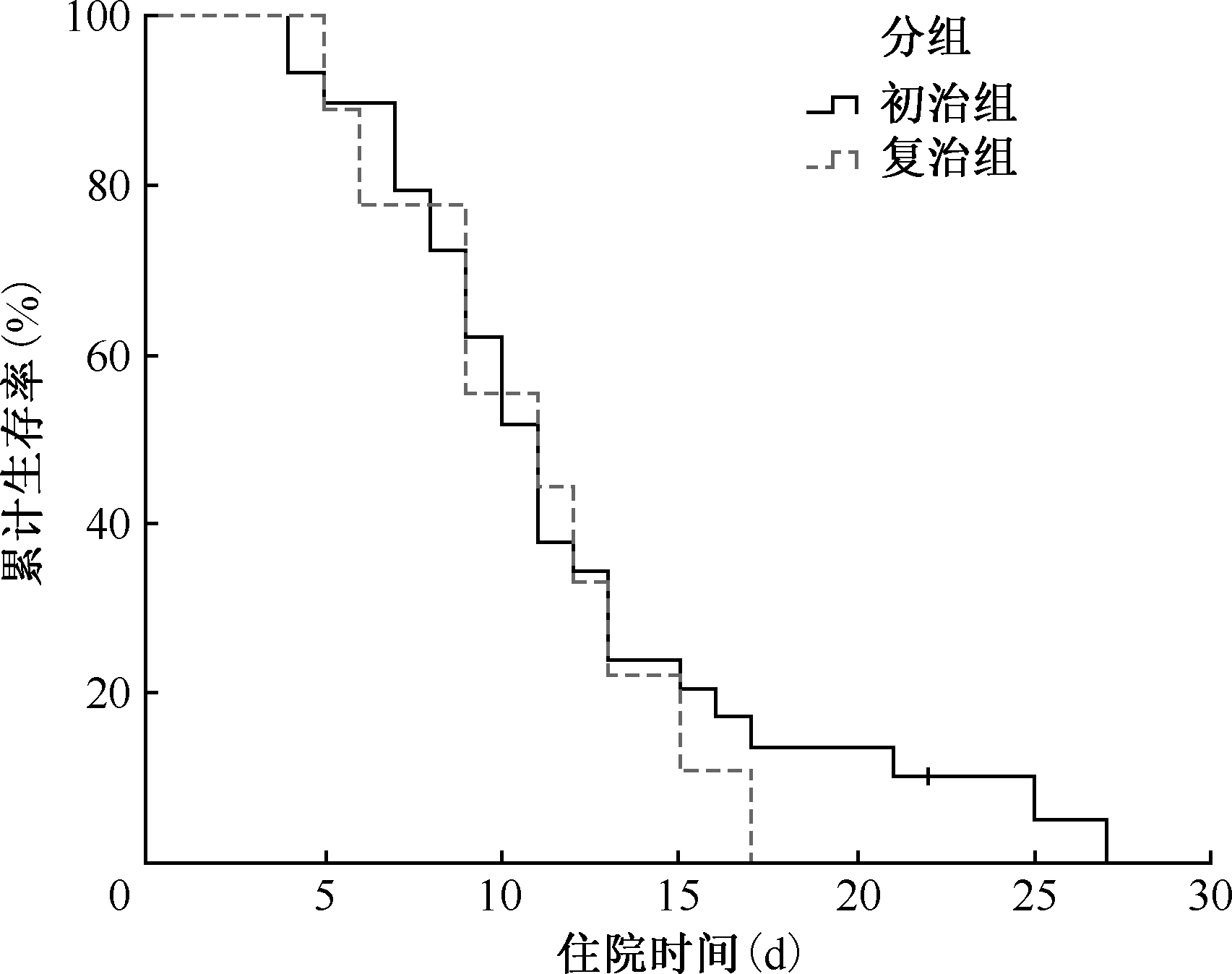
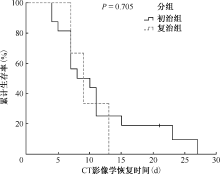
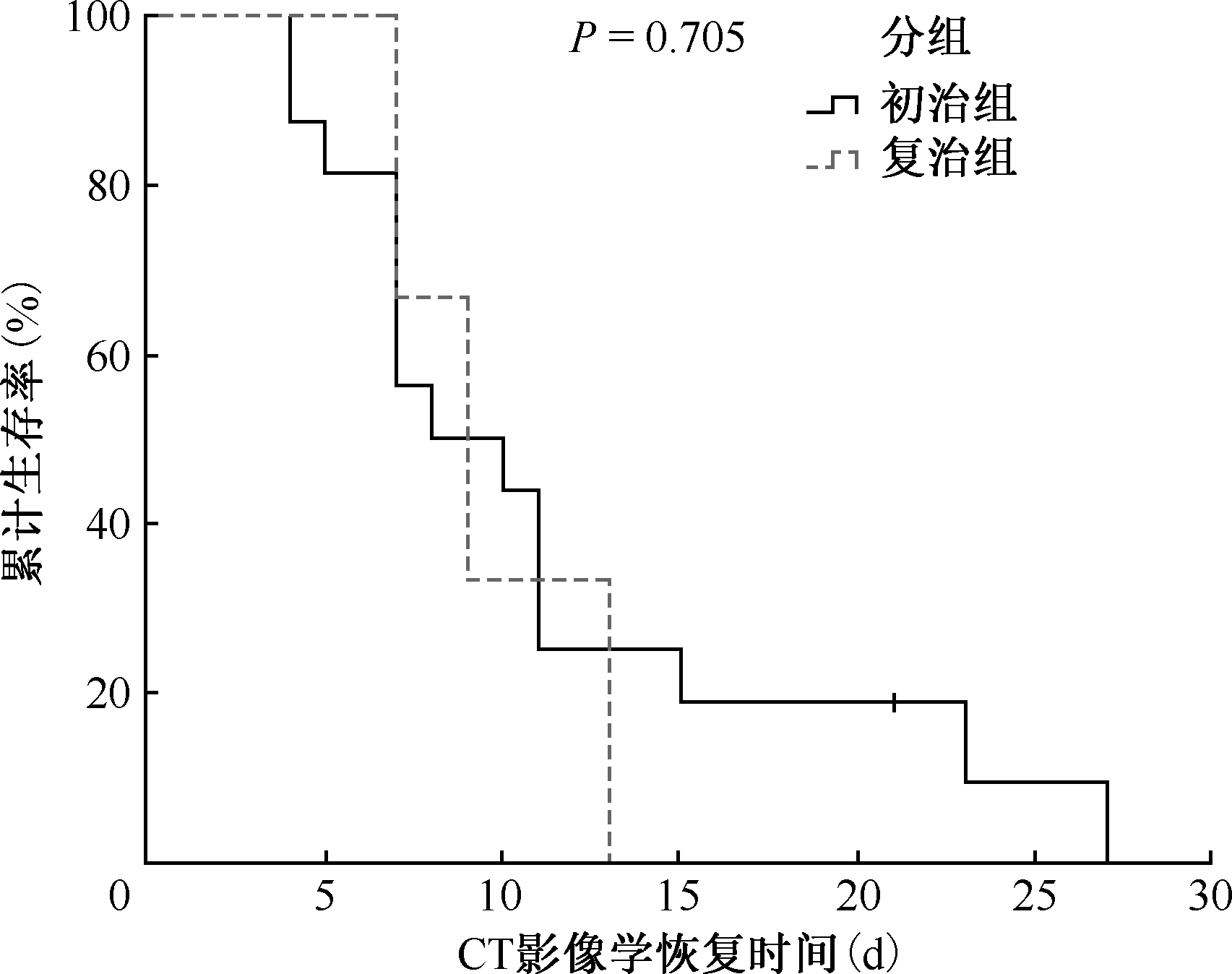
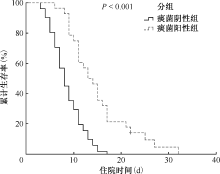
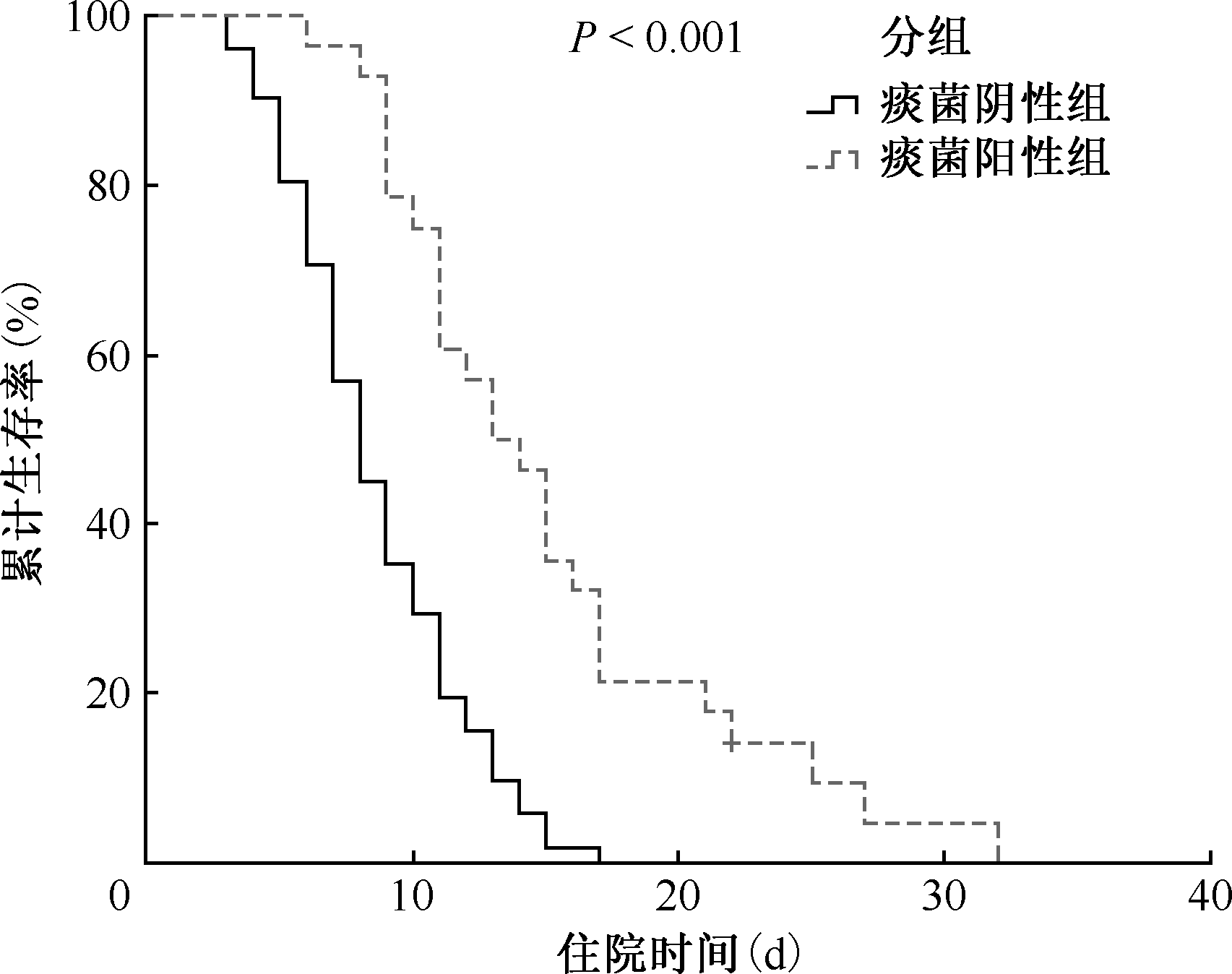
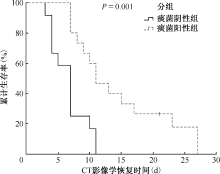
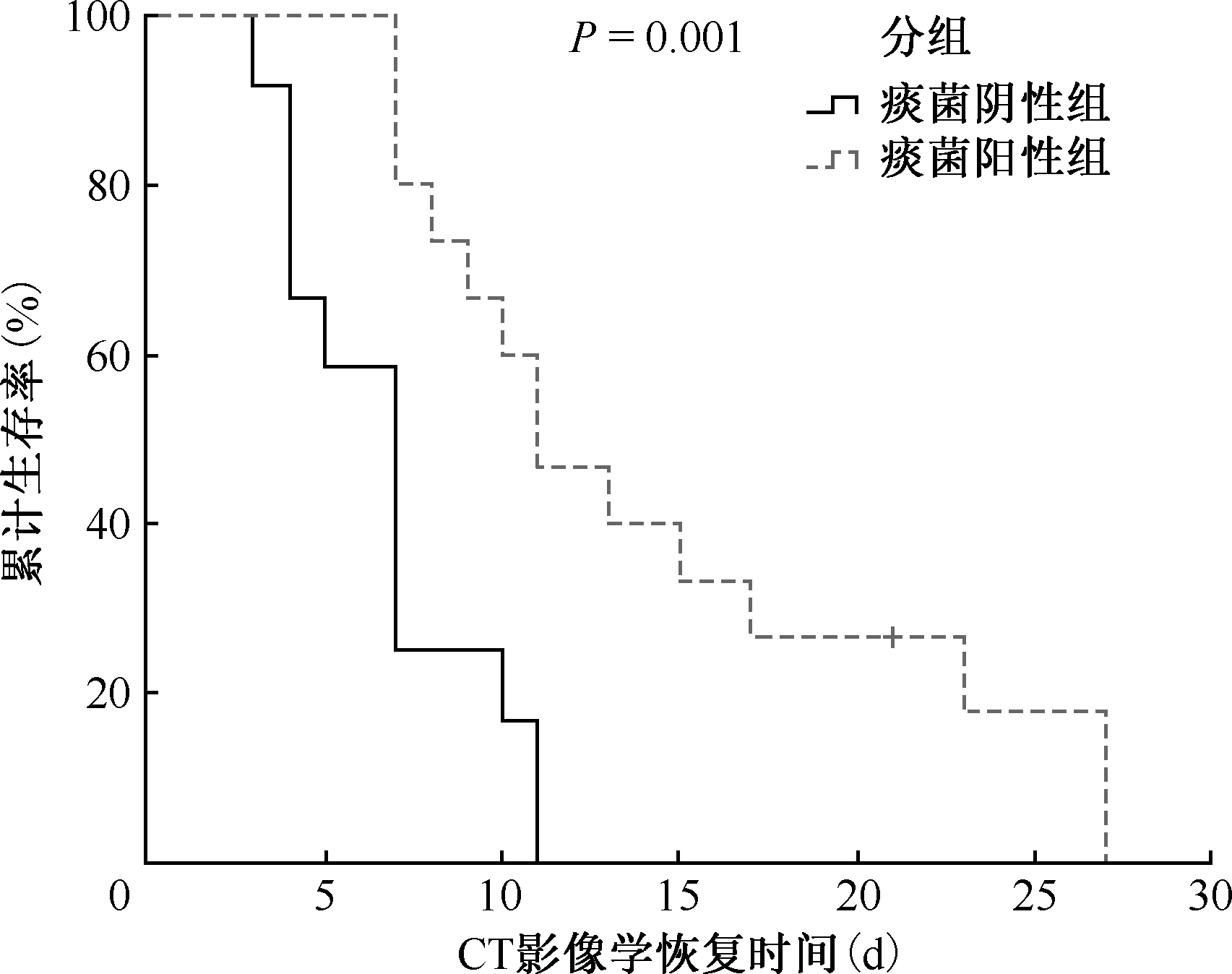
目的: 分析新型冠状病毒(简称“新冠病毒”)感染合并肺结核患者的临床表现、影像学特征及实验室检查指标情况,探讨合并肺结核对新冠病毒感染患者预后的影响。方法: 选取2022年12月至2023年1月于湖南省胸科医院住院并明确诊断为新冠病毒感染的患者作为研究对象,共140例。研究对象中单纯新冠病毒感染患者57例(新冠组);新冠病毒感染合并肺结核患者83例(新冠合并结核组),其中,合并耐药肺结核患者32例。收集研究对象的人口学特征、临床特征、实验室检查结果、预后情况。采用病例-对照设计,首先根据研究对象是否合并肺结核,将其分为新冠组和新冠合并结核组,比较两组研究对象的人口学特征、临床表现、实验室检查结果及预后情况;然后,将新冠合并结核组按照是否耐药、是否痰菌阳性、治疗分类进行分层分析。采用Kaplan-Meierr(KM)生存分析比较组间的生存差异,并进一步探讨影响合并肺结核对新冠病毒感染患者预后的危险因素。结果: 新冠合并结核组的预后更差,CT影像学恢复时间[中位数(四分位数)]为8.5(7.0,11.5)d,与新冠组相比 [7.0(5.0,10.0)d],差异有统计学意义(U=785.000,P=0.049)。新冠合并结核组患者首发症状不典型,发热的患者占38.6%(32/83),低于新冠组(56.1%,32/57),差异有统计学意义(χ2=4.311,P=0.040)。两组患者的影像学表现也有较大差异,新冠组最常出现的是典型磨玻璃影(52.6%,30/57),高于新冠合并结核组的21.7%(18/83),差异有统计学意义(χ2=14.362,P<0.001);新冠合并结核组的影像学表现复杂,最常见的为斑片影(91.6%,76/83)和条索影(91.6%,76/83),高于新冠组的56.1%(32/57)和28.1%(16/57),差异均有统计学意义(χ2值分别为24.052和60.471,P值均<0.001)。新冠合并结核组患者的淋巴细胞计数[中位数(四分位数)]为1.0(0.7,1.6)×109/L,明显低于新冠组的1.3(0.9,2.0)×109/L,差异有统计学意义(U=1736.000,P=0.015);白细胞计数[中位数(四分位数)]为5.0(3.8,7.1)×109/L,明显低于新冠组的6.0(4.8,7.9)×109/L,差异有统计学意义(U=1800.000,P=0.024);中性粒细胞计数[中位数(四分位数)]为3.3(2.2,4.7)×109/L,明显低于新冠组的3.6(3.0,5.2)×109/L,差异有统计学意义(U=1865.000,P=0.049);细胞毒性T细胞(CD3+CD8+)计数[中位数(四分位数)]为344.2(239.6,457.3)/μl,明显低于新冠组的567.6(437.8,618.6)/μl,差异有统计学意义(U=74.000,P=0.009)。生存分析显示,痰菌阳性是影响新冠合并结核患者预后的危险因素。结论: 新冠病毒感染合并肺结核患者住院时间及胸部影像学恢复时间延迟,合并痰菌阳性肺结核的新冠病毒感染患者预后更差。
中图分类号:
 京公网安备11010202007215号
ip访问总数: ip当日访问总数: 当前在线人数:
京公网安备11010202007215号
ip访问总数: ip当日访问总数: 当前在线人数:
 本作品遵循Creative Commons Attribution 3.0 License授权许可
本作品遵循Creative Commons Attribution 3.0 License授权许可