Email Alert | RSS 帮助

中国防痨杂志 ›› 2020, Vol. 42 ›› Issue (3): 266-271.doi: 10.3969/j.issn.1000-6621.2020.03.016
陈振华,刘彬彬,陈忠南,谭云洪( )
)
CHEN Zhen-hua,LIU Bin-bin,CHEN Zhong-nan,TAN Yun-hong()
摘要:
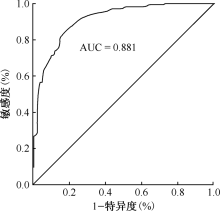
目的 建立病原学阴性初治肺结核患者的诊断模型, 以提高临床诊断的规范性及准确性。方法 收集 2017 年 8 月至 2019 年7 月湖南省胸科医院收治的年龄≥15岁、结核分枝杆菌病原学检查阴性, 且从未因结核病应用过抗结核药物治疗或不规范化疗未满1个月已确诊的200例病原学阴性初治肺结核患者和212例非结核性肺部疾病患者的临床资料。采用简单随机数字表法将两组患者分为两类, 一类为训练样本, 一类为考核样本, 两类样本比例为3∶1。通过对训练样本临床观察指标进行单因素和多因素非条件logistic回归分析, 筛选出独立预测因子并建立诊断模型, 并以训练样本的临床诊断结果为金标准, 采用受试者工作特征(ROC)曲线评估模型的诊断能力, 再使用考核样本对建立的诊断模型进行前瞻性考核。结果 对训练样本临床观察指标的多因素非条件logistic回归分析显示, 血清白蛋白/球蛋白比值(A/G)> 1.2、血清糖类抗原-125(CA-125)> 35kU/L、全血结核分枝杆菌γ-干扰素释放试验(IGRA)阳性、咳嗽≥2周、有咯血或者痰中带血、全身结核中毒症状、并发其他疾病、病灶发生于单侧或两侧的肺上叶尖后段和(或)下叶背段和空洞形成是病原学阴性初治肺结核与非结核性肺部疾病鉴别的相关独立因素[Wald χ 2= 7.264, P= 0.007, OR(95%CI)= 3.433(1.400~8.417); Wald χ 2= 17.114, P= 0.000, OR(95%CI)= 6.980(2.780~17.524); Wald χ 2= 63.643, P= 0.000, OR(95%CI)= 19.283(9.320~39.894); Wald χ 2= 5.557, P= 0.018, OR(95%CI)= 0.434(0.217~0.869); Wald χ 2= 6.237, P= 0.013, OR(95%CI)= 0.255(0.087~0.745); Wald χ 2= 24.930, P= 0.000, OR(95%CI)= 0.126(0.056~0.284); Wald χ 2= 12.062, P= 0.001, OR(95%CI)= 10.139(2.743~37.746); Wald χ 2= 16.224, P= 0.000, OR(95%CI)= 4.428(2.147~9.135); Wald χ 2=16.228, P=0.000, OR(95%CI)=14.437(3.939~52.919)]。ROC曲线分析模型的诊断效能为曲线下面积(AUC)=0.881(95%CI:0.839~0.915), 最佳临界值为0.42, 诊断病原学阴性初治肺结核的敏感度和特异度分别为86.67%和76.10%。经考核样本检验, 建立的诊断模型对两组患者总的准确判别率为79.61%(82/103)。结论 本研究建立的模型敏感度和准确率均较高, 可以作为临床医师诊断病原学阴性初治肺结核的辅助参考工具。
 京公网安备11010202007215号
ip访问总数: ip当日访问总数: 当前在线人数:
京公网安备11010202007215号
ip访问总数: ip当日访问总数: 当前在线人数:
 本作品遵循Creative Commons Attribution 3.0 License授权许可
本作品遵循Creative Commons Attribution 3.0 License授权许可