Email Alert | RSS 帮助

中国防痨杂志 ›› 2026, Vol. 48 ›› Issue (6): 769-778.doi: 10.19982/j.issn.1000-6621.20250503
范佳画1, 颜亮2, 陈华3, 卢春丽1, 汪敏3, 黄亚玲1, 李艳3( )
)
Fan Jiahua1, Yan Liang2, Chen Hua3, Lu Chunli1, Wang Min3, Huang Yaling1, Li Yan3()
摘要:
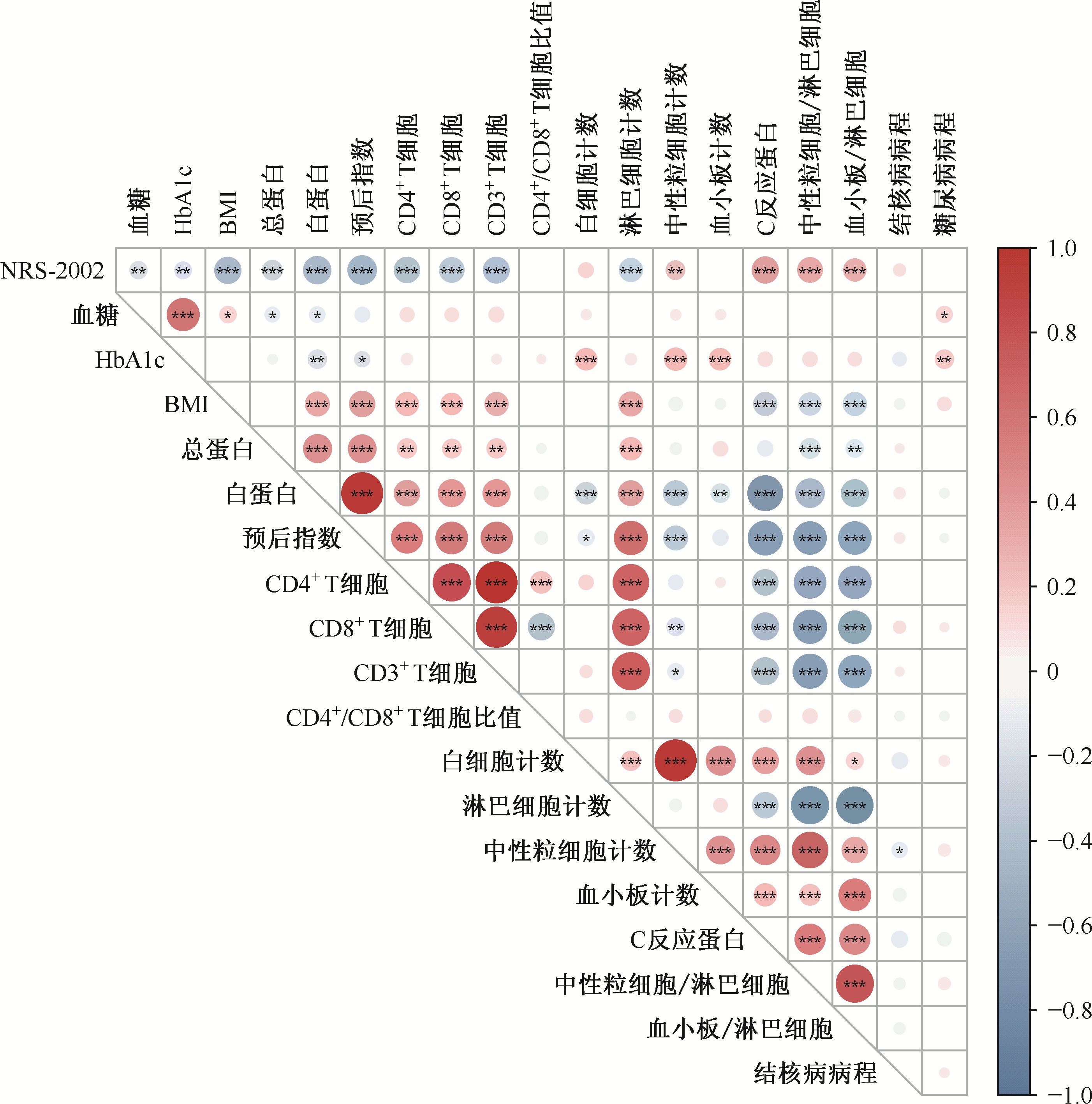
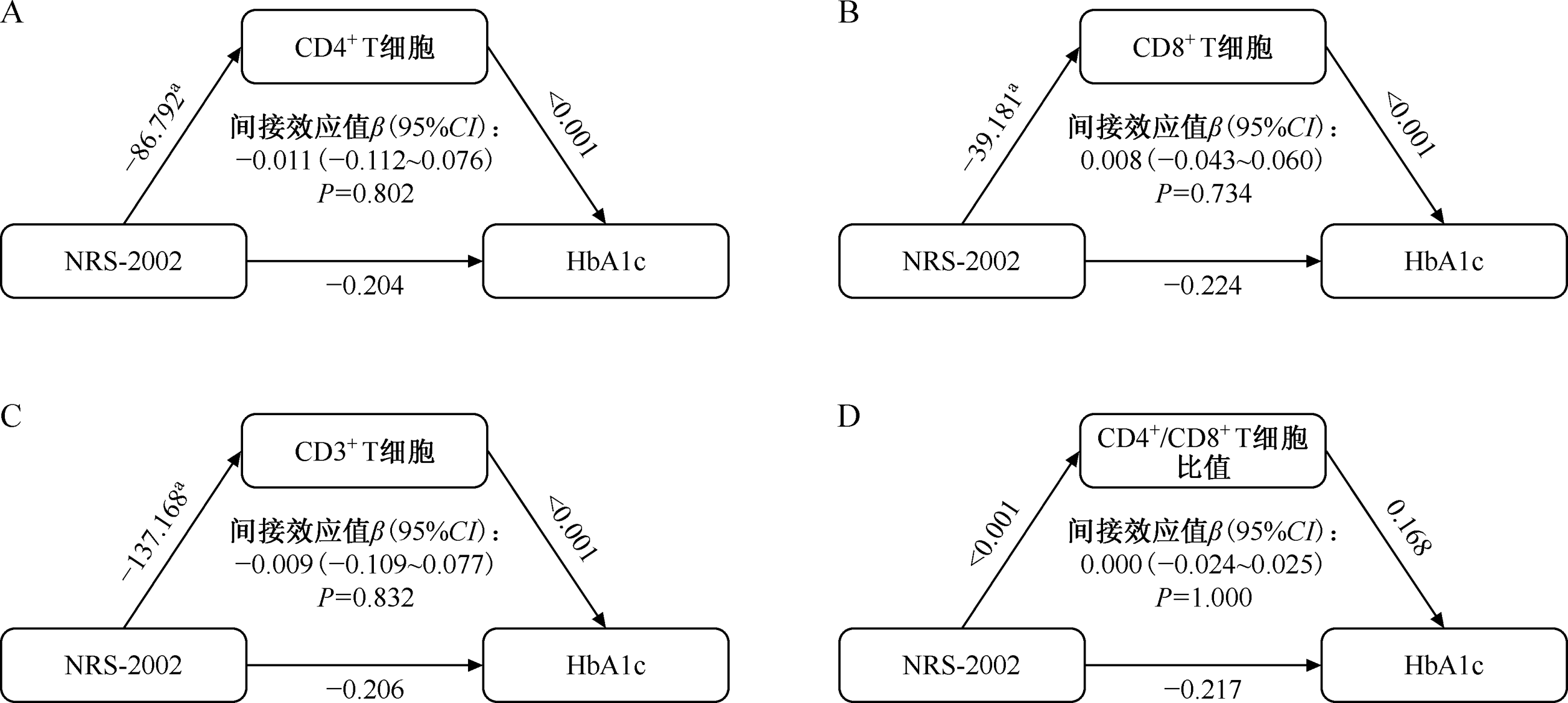
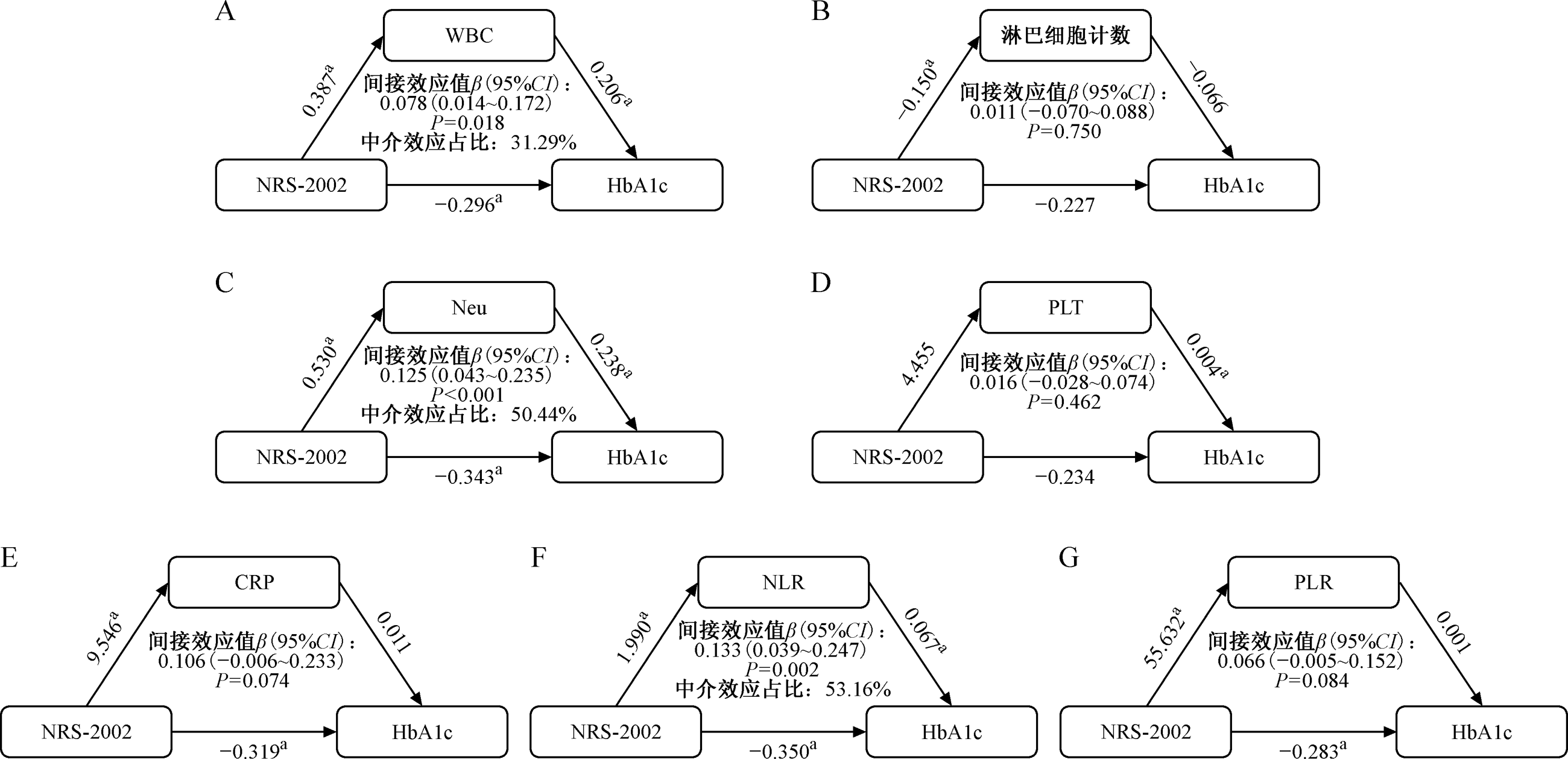
目的: 探讨结核病与糖尿病共病(TB-DM)患者营养风险、炎症指标与血糖控制的关系,为优化TB-DM患者的综合管理提供依据。方法: 采用横断面研究设计,纳入2023年1—12月广州市胸科医院收治的264例TB-DM患者。根据营养风险筛查2002(NRS-2002)评分和糖化血红蛋白(HbA1c)水平进行分组比较。收集患者的营养指标[如体质量指数(BMI)、白蛋白(ALB)、预后营养指数(PNI)]、免疫炎症指标[如CD细胞系列、白细胞计数(WBC)、中性粒细胞计数(Neu)、淋巴细胞计数(LYM)、中性粒细胞与淋巴细胞比值(NLR)、血小板与淋巴细胞比值(PLR)等]及血糖指标(随机血糖和HbA1c)。采用多因素logistic回归分析营养风险与血糖控制不佳的关联,并进一步运用中介效应分析炎症指标在营养风险与血糖控制间的中介作用。结果: 存在营养风险(NRS-2002≥3分)的患者占50.4%(133/264)。与无营养风险组相比,有营养风险组患者的营养及免疫指标均明显降低,如BMI[20.20(18.73,22.95)kg/m2和22.14(20.55,24.22)kg/m2,Z=-4.759,P<0.001]、ALB[(30.93±7.02)g/L和(36.48±7.08) g/L,t=6.393,P<0.001]、CD4+ T细胞计数[392(260,560)个/μl和564(394,756)个/μl,Z=-5.108,P<0.001],且痰涂片阳性率更高[60.90%(81/133)和39.69%(52/131),χ2=11.874,P<0.001]。有营养风险组患者炎症水平明显升高,如NLR[5.20(3.54,10.14)和3.64(2.61,5.48),Z=-4.510,P<0.001]、C反应蛋白[22.54(6.36,58.32)mg/L和5.23(1.36,22.12)mg/L,Z=-4.852,P<0.001],但HbA1c水平反而较低[7.50%(6.60%,10.00%)和8.60%(7.35%,10.20%),Z=-2.711,P=0.007]。多因素logistic回归分析结果表明,在校正混杂因素后,营养风险与血糖控制不佳呈独立负向关联(OR=0.357, 95%CI: 0.194~0.656)。中介效应分析显示,炎症指标(WBC、Neu、NLR)是营养风险影响HbA1c水平的显著中介变量,中介效应占比分别为31.29%、50.44%和53.16%。结论: 在TB-DM患者中,存在营养风险者往往伴有更严重的炎症状态和免疫抑制,但其血糖水平可能因机体严重消耗而相对更低。炎症是连接营养风险与血糖控制的关键路径。临床在管理TB-DM患者时,应在积极控制血糖的基础上,高度重视营养评估,并将调控炎症作为综合治疗的重要环节。
中图分类号:
 京公网安备11010202007215号
ip访问总数: ip当日访问总数: 当前在线人数:
京公网安备11010202007215号
ip访问总数: ip当日访问总数: 当前在线人数:
 本作品遵循Creative Commons Attribution 3.0 License授权许可
本作品遵循Creative Commons Attribution 3.0 License授权许可