Email Alert | RSS 帮助

中国防痨杂志 ›› 2023, Vol. 45 ›› Issue (12): 1170-1176.doi: 10.19982/j.issn.1000-6621.20230287
张文倩1,2, 黄飞3, 张国钦2, 庞学文2, 张帆2( )
)
Zhang Wenqian1,2, Huang Fei3, Zhang Guoqin2, Pang Xuewen2, Zhang Fan2()
摘要:
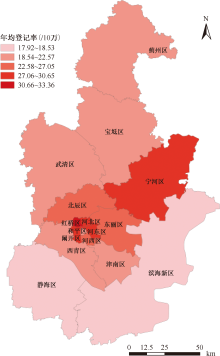
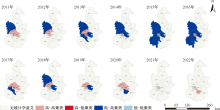
目的: 分析2011—2022年天津市肺结核时空分布特征和聚集性,为提高天津市肺结核防治工作水平、制定区域性结核病控制策略提供理论依据。方法: 通过“中国疾病预防控制信息系统”子系统“结核病管理信息系统”和天津市统计年鉴及“中国传染病监测信息报告管理系统”获得2011—2022年登记报告现住址为天津市的肺结核登记率、患者资料(患者发病登记时间和现住址)、行政区域,以及天津市相关人口学信息。采用SPSS 26.0、ArcGIS 10.7和SaTScan 10.1软件对天津市肺结核登记率进行全局和局部空间自相关及时空扫描聚集性分析。结果: 2011—2022年天津市肺结核登记率介于20.40/10万(2801/13730000)~26.42/10万(3543/13410000),差异无统计学意义($x^{2}_{趋势}=1.144$,P=0.233),年均登记率为23.82/10万(39907/167506000),年均递降率为2.32%$\left[\left(\sqrt[11]{\frac{20.40}{26.42}}-1\right) \times 100 \%\right]$。2012—2016年肺结核年登记率在23.15/10万(3190/13780000)~25.16/10万(3548/14100000)之间,存在空间聚集性(Moran’s I指数=0.138、0.228、0.130、0.238和0.288,Z=2.474、3.625、2.417、3.732和4.368,P=0.013、<0.001、0.016、<0.001和<0.001)。局部空间自相关分析显示,天津市仅2021年未形成各地区肺结核聚集区,其他年份均形成高-高(HH)和低-高(LH)两种聚集模式,其中,高-高聚集主要集中在市内六区(和平区、河西区、河东区、南开区、河北区、红桥区)和环城四区(北辰区、东丽区、西青区、津南区)。时空扫描结果显示存在2个聚集区,一级聚集区主要集中在2011—2016年的市内六区(LLR=383.11,RR=1.42,P<0.001),二级聚集区集中在2014—2019年的滨海新区(LLR=27.12,RR=1.32,P<0.001)。结论: 2011—2022年天津市肺结核疫情趋于稳定,但在2012—2016年间存在空间聚集性,高-高聚集多集中在市内六区和环城四区,且在市内六区和滨海新区出现时空聚集性,应关注人口流动性大、人口稠密和经济发展重心地区的结核病疫情变化,提高地区诊断鉴别水平和探索主动发现策略,因地制宜调整结核病防治策略。
中图分类号:
 京公网安备11010202007215号
ip访问总数: ip当日访问总数: 当前在线人数:
京公网安备11010202007215号
ip访问总数: ip当日访问总数: 当前在线人数:
 本作品遵循Creative Commons Attribution 3.0 License授权许可
本作品遵循Creative Commons Attribution 3.0 License授权许可