
Chinese Journal of Antituberculosis ›› 2024, Vol. 46 ›› Issue (6): 687-698.doi: 10.19982/j.issn.1000-6621.20240127
• Original Articles • Previous Articles Next Articles
Li Yao, Fang Zhe, Luo Danlin, Hu Yanmei, Tang Mi, Tang Zhigang, Wen Xinmin, Zhang Yong, Yao Bibo, Wang Qi, Yi Hengzhong( )
)
Received:2024-04-03
Online:2024-06-10
Published:2024-06-03
Contact:
Yi Hengzhong, Email: Supported by:CLC Number:
Li Yao, Fang Zhe, Luo Danlin, Hu Yanmei, Tang Mi, Tang Zhigang, Wen Xinmin, Zhang Yong, Yao Bibo, Wang Qi, Yi Hengzhong. Clinical characteristics and prognosis of patients with novel coronavirus infection complicated with pulmonary tuberculosis[J]. Chinese Journal of Antituberculosis, 2024, 46(6): 687-698. doi: 10.19982/j.issn.1000-6621.20240127
Add to citation manager EndNote|Ris|BibTeX
URL: https://www.zgflzz.cn/EN/10.19982/j.issn.1000-6621.20240127
| 特征 | 合计 (140例) | 新冠组 (57例) | 新冠合并结核组 (83例) | 统计 检验值 | P值 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 年龄(岁,$\bar{x}±s$) | 61.3±16.9 | 64.8±17.6 | 58.9±16.1 | t=2.080 | 0.039 | ||||||||||
| 性别[例(构成比,%)] | χ2=8.667 | 0.003 | |||||||||||||
| 男性 | 89(63.6) | 28(49.1) | 61(73.5) | ||||||||||||
| 女性 | 51(36.4) | 29(50.9) | 22(26.5) | ||||||||||||
| 体质量指数($\bar{x}±s$) | 21.9±4.0 | 23.8±3.7 | 20.7±3.8 | t=4.721 | <0.001 | ||||||||||
| 吸烟[例(构成比,%)] | χ2=7.851 | 0.006 | |||||||||||||
| 是 | 48(34.3) | 12(21.1) | 36(43.4) | ||||||||||||
| 否 | 92(65.7) | 45(78.9) | 47(56.6) | ||||||||||||
| 饮酒[例(构成比,%)] | χ2=0.760 | 0.383 | |||||||||||||
| 是 | 19(13.6) | 6(10.5) | 13(15.7) | ||||||||||||
| 否 | 121(86.4) | 51(89.5) | 70(84.3) | ||||||||||||
| 预后情况[例(构成比,%)] | χ2=0.002 | 0.961 | |||||||||||||
| 改善 | 135(96.4) | 55(96.5) | 80(96.4) | ||||||||||||
| 恶化 | 5(3.6) | 2(3.5) | 3(3.6) | ||||||||||||
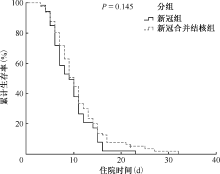
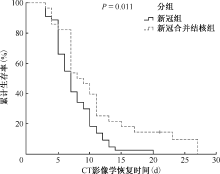
| 住院时间[d,M(Q1,Q3)] | 10.0(7.0,13.0) | 9.5(6.0,12.0) | 10.0(7.0,13.0) | U=2398.000 | 0.251 | ||||||||||
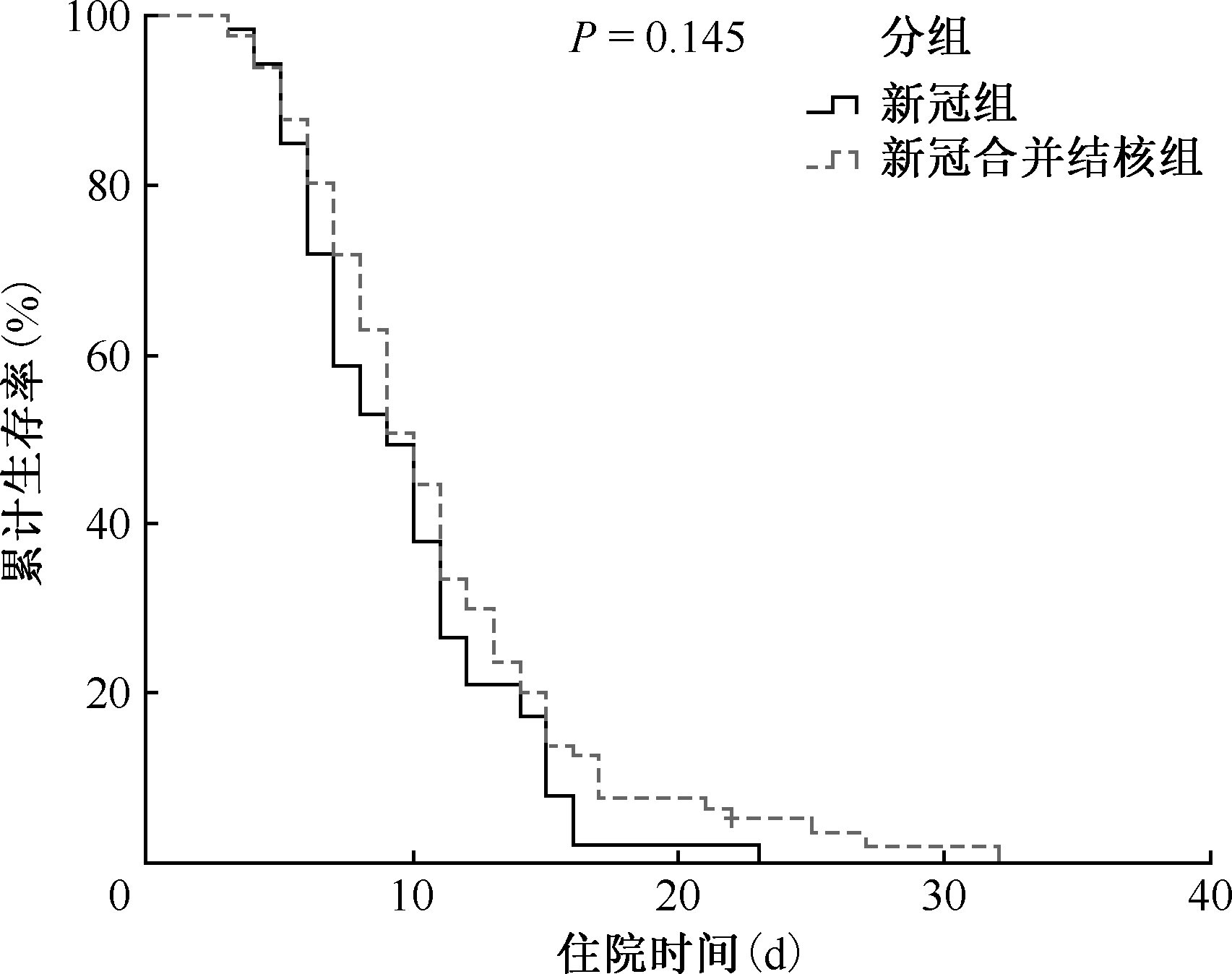
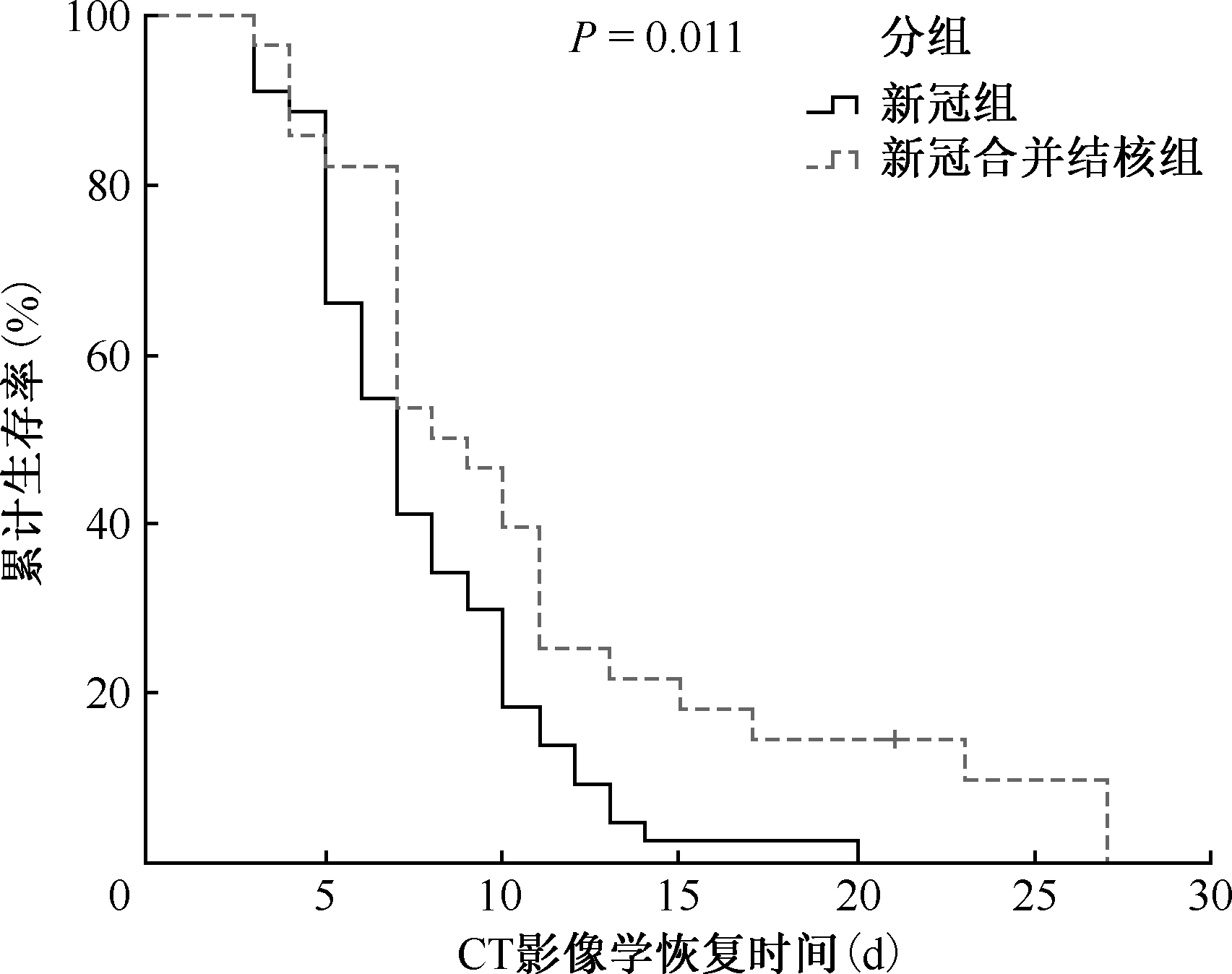
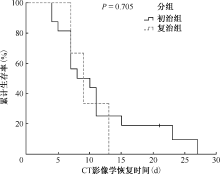
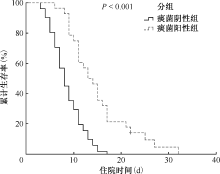
| CT影像学恢复时间[d,M(Q1,Q3)] | 7.0(5.0,11.0) | 7.0(5.0,10.0) | 8.5(7.0,11.5) | U=785.000 | 0.049 | ||||||||||
| 合并症[例(发生率,%)] | |||||||||||||||
| 尘肺 | 6(5.2) | 0(0.0) | 6(7.6) | χ2=1.617 | 0.203 | ||||||||||
| 慢性阻塞性肺疾病 | 57(49.1) | 19(51.4) | 38(48.1) | χ2=0.107 | 0.744 | ||||||||||
| 肿瘤 | 5(4.2) | 3(7.7) | 2(2.5) | χ2=0.678 | 0.410 | ||||||||||
| 糖尿病 | 31(25.6) | 7(17.1) | 24(30.0) | χ2=2.377 | 0.123 | ||||||||||
| 心血管疾病 | 61(50.0) | 27(62.8) | 34(43.0) | χ2=4.346 | 0.037 | ||||||||||
| 慢性肝病 | 6(5.2) | 1(2.7) | 5(6.3) | χ2=0.139 | 0.710 | ||||||||||
| 慢性肾病 | 1(0.9) | 0(0.0) | 1(1.3) | 1.000a | |||||||||||
| 首发症状[例(发生率,%)] | |||||||||||||||
| 发热 | 64(45.7) | 32(56.1) | 32(38.6) | χ2=4.211 | 0.040 | ||||||||||
| 咳嗽 | 125(89.3) | 53(93.0) | 72(86.7) | χ2=1.373 | 0.241 | ||||||||||
| 呼吸困难 | 63(45.0) | 26(45.6) | 37(44.6) | χ2=0.015 | 0.904 | ||||||||||
| 肌肉酸痛 | 24(17.1) | 9(15.8) | 15(18.1) | χ2=0.124 | 0.725 | ||||||||||
| 咽痛 | 20(14.3) | 8(14.0) | 12(14.5) | χ2=0.005 | 0.944 | ||||||||||
| 胸闷 | 21(15.0) | 9(15.8) | 12(14.5) | χ2=0.047 | 0.828 | ||||||||||
| 消化道症状 | 36(25.7) | 12(21.1) | 24(28.9) | χ2=1.094 | 0.296 | ||||||||||
| 皮肤症状 | 2(1.4) | 0(0.0) | 2(2.4) | 0.514a | |||||||||||
| CT影像学特征[例(发生率,%)] | |||||||||||||||
| 磨玻璃影 | 48(34.3) | 30(52.6) | 18(21.7) | χ2=14.362 | <0.001 | ||||||||||
| 斑片影 | 108(77.1) | 32(56.1) | 76(91.6) | χ2=24.052 | <0.001 | ||||||||||
| 条索影 | 92(65.7) | 16(28.1) | 76(91.6) | χ2=60.471 | <0.001 | ||||||||||
| 胸膜增厚 | 29(20.7) | 4(7.0) | 25(30.1) | χ2=10.982 | 0.001 | ||||||||||
| 结节 | 31(22.1) | 7(12.3) | 24(28.9) | χ2=5.424 | 0.020 | ||||||||||
| 淋巴结肿大 | 25(17.9) | 3(5.3) | 22(26.5) | χ2=10.396 | 0.001 | ||||||||||
| 累及双肺 | 112(80.0) | 49(86.0) | 63(75.9) | χ2=2.138 | 0.144 | ||||||||||
| 累及右肺 | 13(9.3) | 5(8.8) | 8(9.6) | χ2=0.030 | 0.862 | ||||||||||
| 累及左肺 | 15(10.7) | 3(5.3) | 12(14.5) | χ2=2.986 | 0.084 | ||||||||||
| 治疗方案[例(使用率,%)] | |||||||||||||||
| 抗生素治疗 | 92(65.7) | 47(82.5) | 45(54.2) | χ2=11.961 | 0.001 | ||||||||||
| 中药治疗 | 81(57.9) | 32(56.1) | 49(59.0) | χ2=0.116 | 0.733 | ||||||||||
| 激素治疗 | 25(17.9) | 16(28.1) | 9(10.8) | χ2=6.837 | 0.009 | ||||||||||
| 激素治疗时间[d,M(Q1,Q3)] | 6.0(4.0,8.0) | 6.0(3.8,8.0) | 6.0(4.0,11.0) | U=80.500 | 0.637 | ||||||||||
| 抗病毒治疗 | 24(17.1) | 14(24.6) | 10(12.0) | χ2=3.725 | 0.054 | ||||||||||
| 抗病毒治疗时间[d,M(Q1,Q3)] | 7.0(7.0,7.0) | 7.0(6.5,8.3) | 7.0(5.5,12.3) | U=67.000 | 0.850 | ||||||||||
| 实验室检测指标 | |||||||||||||||
| 红细胞计数[×1012/L,M(Q1,Q3)] | 4.2(3.8,4.6) | 4.2(3.9,4.6) | 4.1(3.7,4.5) | U=1941.000 | 0.124 | ||||||||||
| 血红蛋白(g/L,$\bar{x}±s$) | 120.8±18.6 | 124.5±16.5 | 118.3±19.6 | t=2.007 | 0.047 | ||||||||||
| 红细胞压积(%,$\bar{x}±s$) | 36.1±5.3 | 37.4±4.7 | 35.2±5.5 | t=2.488 | 0.014 | ||||||||||
| 血小板计数(×109/L,$\bar{x}±s$) | 215.5±92.7 | 223.5±95.8 | 210.1±90.7 | t=0.831 | 0.407 | ||||||||||
| 淋巴细胞计数[×109/L,M(Q1,Q3)] | 1.1(0.8,1.7) | 1.3(0.9,2.0) | 1.0(0.7,1.6) | U=1736.000 | 0.015 | ||||||||||
| 白细胞计数[×109/L,M(Q1,Q3)] | 5.4(4.0,7.6) | 6.0(4.8,7.9) | 5.0(3.8,7.1) | U=1800.000 | 0.024 | ||||||||||
| 中性粒细胞计数[×109/L, M(Q1,Q3)] | 3.4(2.5,5.1) | 3.6(3.0,5.2) | 3.3(2.2,4.7) | U=1865.500 | 0.049 | ||||||||||
| 中性粒细胞百分比[%,M(Q1,Q3)] | 63.4(54.6,74.3) | 62.4(55.7,75.0) | 64.1(52.8,73.8) | U=2264.500 | 0.798 | ||||||||||
| CD3+CD4+细胞计数[个/μl, M(Q1,Q3)] | 545.1(396.6,781.8) | 703.7(535.3,800.6) | 454.7(301.3,638.6) | U=107.000 | 0.142 | ||||||||||
| CD3+CD4+细胞百分比[%, M(Q1,Q3)] | 37.1(32.2,45.7) | 36.4(32.1,44.6) | 39.1(33.4,47.7) | U=172.000 | 0.523 | ||||||||||
| CD3+CD8+细胞计数[个/μl, M(Q1,Q3)] | 436.8(247.9,575.4) | 567.6(437.8,618.6) | 344.2(239.6,457.3) | U=74.000 | 0.009 | ||||||||||
| CD3+CD8+细胞百分比[%, M(Q1,Q3)] | 25.5(21.2,34.4) | 26.8(22.2,34.4) | 24.7(18.2,34.7) | U=126.000 | 0.403 | ||||||||||
| CD4+/CD8+比值[M(Q1,Q3)] | 1.5(1.0,2.0) | 1.3(1.1,1.7) | 1.7(1.0,2.7) | U=178.000 | 0.403 | ||||||||||
| CD3+/CD16+CD56+细胞计数[个/μl,M(Q1,Q3)] | 227.8(121.3,415.0) | 252.4(155.5,495.3) | 193.8(105.1,393.8) | U=114.000 | 0.217 | ||||||||||
| CD3+/CD16+CD56+细胞百分比[%,M(Q1,Q3)] | 16.6(11.1,22.9) | 16.7(10.4,22.7) | 16.6(12.0,24.8) | U=153.000 | 1.000 | ||||||||||
| CD3+CD19+细胞计数[个/μl, M(Q1,Q3)] | 160.0(83.4,218.5) | 174.3(145.9,217.2) | 127.7(63.4,214.5) | U=108.000 | 0.151 | ||||||||||
| CD3+CD19+细胞百分比[%, M(Q1,Q3)] | 10.2(7.8,14.3) | 10.7(8.0,12.4) | 8.9(6.3,14.5) | U=133.000 | 0.545 | ||||||||||
| CD3+CD45+细胞计数[个/μl, M(Q1,Q3)] | 956.9(761.9,1421.6) | 1293.4(923.3,1475.9) | 841.0(662.8,1162.9) | U=93.000 | 0.052 | ||||||||||
| CD3+CD45+细胞百分比[%, M(Q1,Q3)] | 69.0(63.8,74.3) | 71.3(64.5,74.1) | 67.8(63.8,74.6) | U=145.000 | 0.832 | ||||||||||
| C反应蛋白[mg/L,M(Q1,Q3)] | 9.7(3.3,34.9) | 8.6(3.0,42.7) | 9.7(4.8,34.8) | U=2248.000 | 0.784 | ||||||||||
| 降钙素原[ng/ml,M(Q1,Q3)] | 0.0(0.0,0.1) | 0.0(0.0,0.2) | 0.0(0.0,0.1) | U=2203.000 | 0.690 | ||||||||||
| 血红细胞沉降率[mm/1h, M(Q1,Q3)] | 29.0(14.8,48.0) | 28.0(15.5,46.0) | 29.0(14.0,48.0) | U=2112.500 | 0.982 | ||||||||||
| 谷丙转氨酶[U/L,M(Q1,Q3)] | 15.9(11.0,26.0) | 18.0(11.8,27.4) | 14.9(10.4,23.9) | U=1965.500 | 0.152 | ||||||||||
| 谷草转氨酶[U/L,M(Q1,Q3)] | 30.0(23.8,38.0) | 30.3(23.0,38.3) | 30.0(23.9,38.0) | U=2324.000 | 0.903 | ||||||||||
| 总胆红素[μmol/L,M(Q1,Q3)] | 10.2(7.5,13.8) | 10.4(8.3,13.8) | 10.1(7.5,13.8) | U=2172.000 | 0.591 | ||||||||||
| 内生肌酐清除率[ml/min, M(Q1,Q3)] | 78.6(62.5,102.6) | 75.6(62.1,99.5) | 81.3(63.4,102.4) | U=2126.000 | 0.429 | ||||||||||
| 活化部分凝血活酶时间[s, M(Q1,Q3)] | 27.8(25.2,30.7) | 26.6(24.8,28.7) | 28.1(26.1,32.1) | U=2890.000 | 0.006 | ||||||||||
| 血浆凝血酶原时间[s,M(Q1,Q3)] | 11.5(10.7,12.6) | 11.4(10.6,12.2) | 11.7(10.8,12.8) | U=2678.500 | 0.072 | ||||||||||
| 凝血酶时间[s,M(Q1,Q3)] | 17.4(16.4,18.3) | 17.6(16.6,18.4) | 17.4(16.3,18.1) | U=2193.500 | 0.744 | ||||||||||
| 心肌肌钙蛋白Ⅰ[ng/ml,M(Q1,Q3)] | 0.05(0.02,0.09) | 0.03(0.02,0.09) | 0.05(0.02,0.08) | U=1897.500 | 0.884 | ||||||||||
| 乳酸脱氢酶[U/L,M(Q1,Q3)] | 178.0(159.3,217.9) | 186.4(166.0,235.5) | 170.3(151.7,205.7) | U=1784.000 | 0.030 | ||||||||||
| 肌酸激酶[U/L,M(Q1,Q3)] | 59.5(41.3,92.0) | 65.0(49.0,102.5) | 56.0(36.0,85.5) | U=1780.500 | 0.029 | ||||||||||
| 肌酸激酶同工酶[U/L,M(Q1,Q3)] | 9.0(7.0,13.0) | 10.5(7.5,13.1) | 8.6(7.0,11.1) | U=1955.000 | 0.154 | ||||||||||
| 特征 | 合计(81例) | 痰菌阴性组(52例) | 痰菌阳性组(29例) | 统计检验值 | P值 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 年龄(岁,$\bar{x}±s$) | 58.9±16.2 | 59.2±16.2 | 58.4±16.5 | t=0.220 | 0.826 | |||||||||
| 性别[例(构成比,%)] | χ2=1.348 | 0.246 | ||||||||||||
| 男性 | 61(75.3) | 37(71.2) | 24(82.8) | |||||||||||
| 女性 | 20(24.7) | 15(28.8) | 5(17.2) | |||||||||||
| 体质量指数($\bar{x}±s$) | 20.7±3.8 | 21.2±4.0 | 19.8±3.4 | t=1.633 | 0.107 | |||||||||
| 吸烟[例(构成比,%)] | χ2=0.123 | 0.726 | ||||||||||||
| 是 | 37(45.7) | 23(44.2) | 14(48.3) | |||||||||||
| 否 | 44(54.3) | 29(55.8) | 15(51.7) | |||||||||||
| 饮酒[例(构成比,%)] | χ2=0.009 | 0.922 | ||||||||||||
| 是 | 13(16.0) | 9(17.3) | 4(13.8) | |||||||||||
| 否 | 68(84.0) | 43(82.7) | 25(86.2) | |||||||||||
| 预后情况[例(构成比,%)] | χ2=0.273 | 0.601 | ||||||||||||
| 改善 | 78(96.3) | 51(98.1) | 27(93.1) | |||||||||||
| 恶化 | 3(3.7) | 1(1.9) | 2(6.9) | |||||||||||
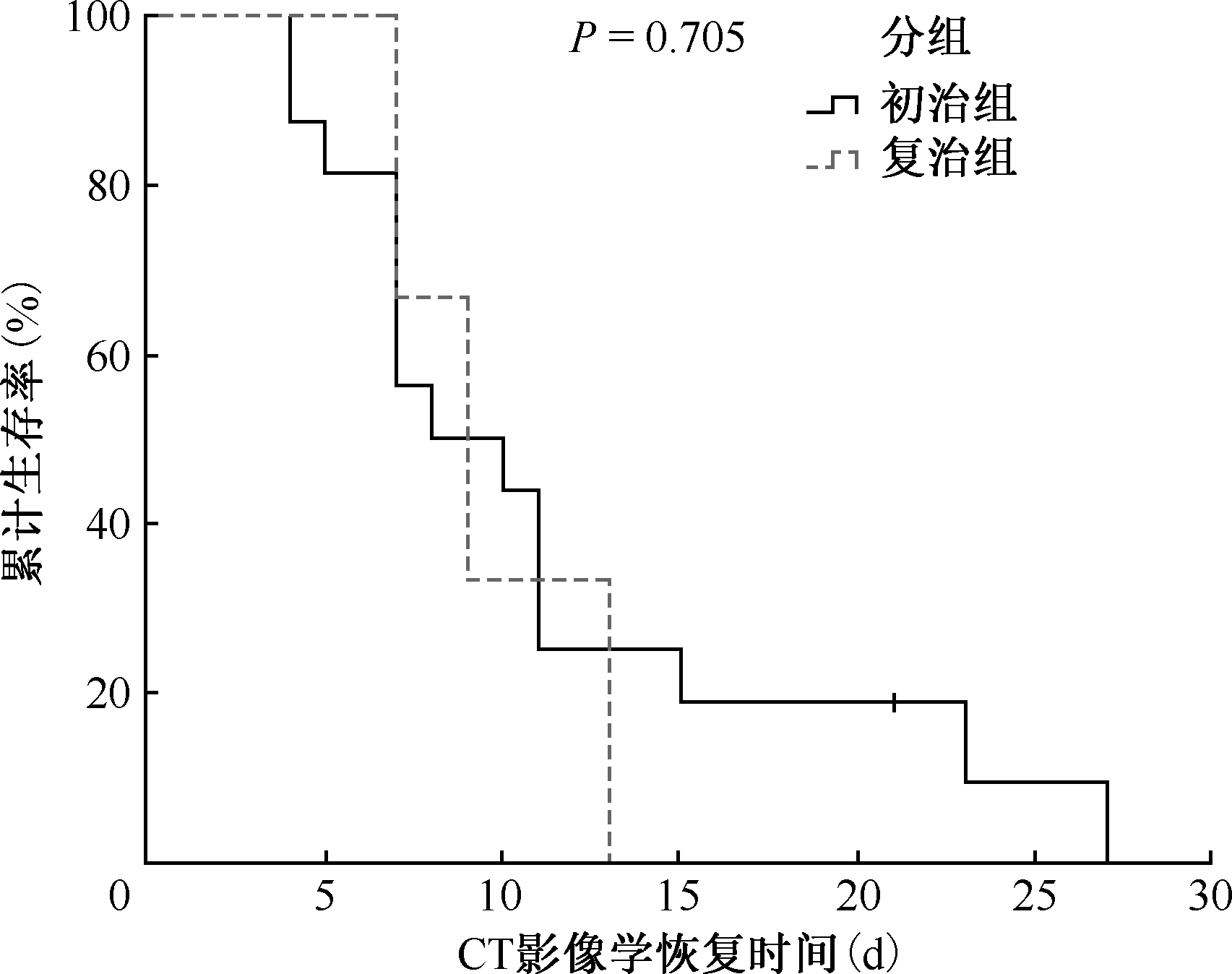
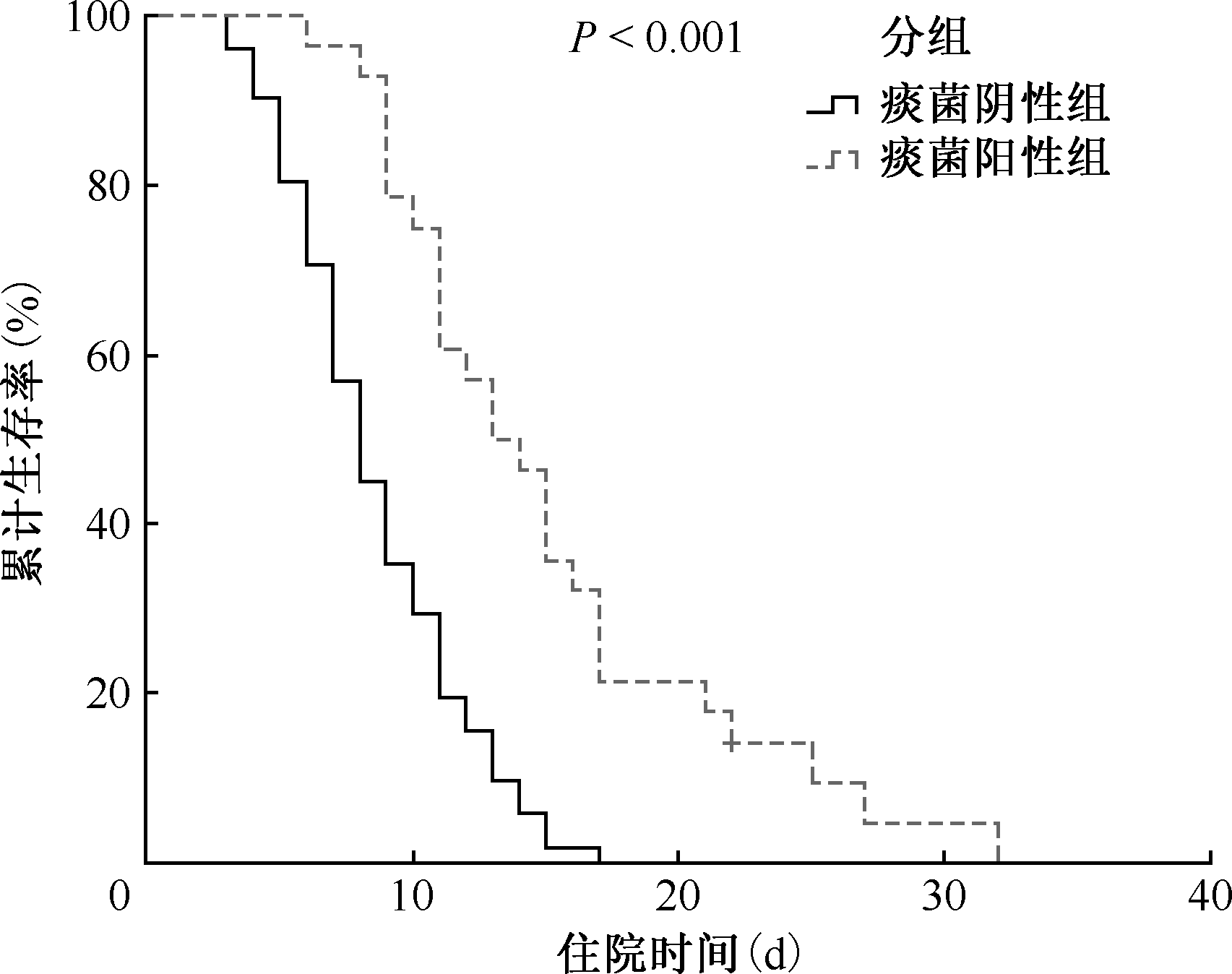
| 住院时间[d,M(Q1,Q3)] | 10.0(7.0,13.0) | 8.0(6.0,11.0) | 13.5(10.8,17.0) | U=1180.500 | <0.001 | |||||||||
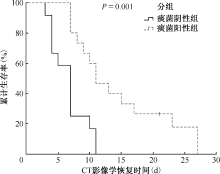
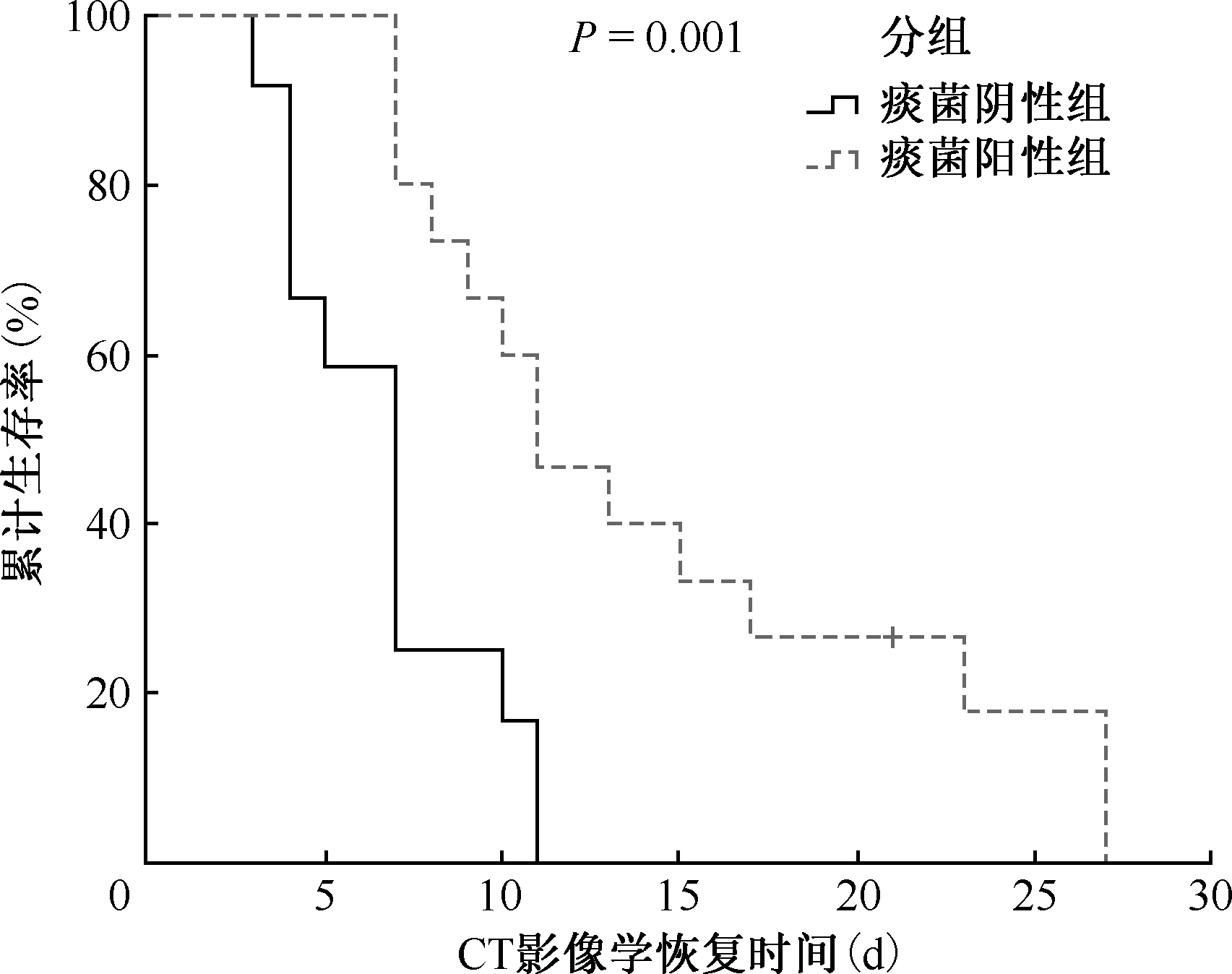
| CT影像学恢复时间[d,M(Q1,Q3)] | 9.0(7.0,12.0) | 7.0(4.0,7.8) | 11.0(8.5,19.0) | U=154.500 | 0.001 | |||||||||
| 合并症[例(发生率,%)] | ||||||||||||||
| 尘肺 | 6(7.8) | 4(7.8) | 2(7.7) | χ2=0.001 | 0.981 | |||||||||
| 慢性阻塞性肺疾病 | 37(48.1) | 24(47.1) | 13(50.0) | χ2=0.060 | 0.807 | |||||||||
| 肿瘤 | 2(2.6) | 1(2.0) | 1(3.8) | 1.000a | ||||||||||
| 糖尿病 | 24(30.8) | 15(28.8) | 9(34.6) | χ2=0.271 | 0.603 | |||||||||
| 心血管疾病 | 33(42.9) | 25(49.0) | 8(30.8) | χ2=2.342 | 0.126 | |||||||||
| 慢性肝病 | 4(5.2) | 3(5.9) | 1(3.8) | χ2=1.987 | 0.159 | |||||||||
| 慢性肾病 | 1(1.3) | 0(0.0) | 1(3.8) | 0.338a | ||||||||||
| 首发症状[例(发生率,%)] | ||||||||||||||
| 发热 | 31(38.3) | 17(32.7) | 14(48.3) | χ2=1.914 | 0.167 | |||||||||
| 咳嗽 | 70(86.4) | 45(86.5) | 25(86.2) | χ2=0.002 | 0.967 | |||||||||
| 呼吸困难 | 37(45.7) | 19(36.5) | 18(62.1) | χ2=4.890 | 0.027 | |||||||||
| 肌肉酸痛 | 14(17.3) | 8(15.4) | 6(20.7) | χ2=0.366 | 0.545 | |||||||||
| 咽痛 | 11(13.6) | 6(11.5) | 5(17.2) | χ2=0.144 | 0.704 | |||||||||
| 胸闷 | 12(14.8) | 8(15.4) | 4(13.8) | χ2=0.000 | 1.000 | |||||||||
| 消化道症状 | 24(29.6) | 17(32.7) | 7(24.1) | χ2=0.653 | 0.419 | |||||||||
| 皮肤症状 | 2(2.5) | 1(1.9) | 1(3.4) | 1.000a | ||||||||||
| CT影像学特征[例(发生率,%)] | ||||||||||||||
| 磨玻璃影 | 18(22.2) | 11(21.2) | 7(24.1) | χ2=0.096 | 0.757 | |||||||||
| 斑片影 | 74(91.4) | 46(88.5) | 28(96.6) | χ2=0.689 | 0.407 | |||||||||
| 条索影 | 74(91.4) | 48(92.3) | 26(89.7) | χ2=0.000 | 1.000 | |||||||||
| 胸膜增厚 | 24(29.6) | 15(28.8) | 9(31.0) | χ2=0.043 | 0.836 | |||||||||
| 结节 | 24(29.6) | 18(34.6) | 6(20.7) | χ2=1.732 | 0.188 | |||||||||
| 淋巴结肿大 | 22(27.2) | 12(23.1) | 10(34.5) | χ2=1.224 | 0.269 | |||||||||
| 累及双肺 | 62(76.5) | 36(69.2) | 26(89.7) | χ2=4.326 | 0.038 | |||||||||
| 累及右肺 | 7(8.6) | 7(13.5) | 0(0.0) | χ2=2.738 | 0.098 | |||||||||
| 累及左肺 | 12(14.8) | 9(17.3) | 3(10.3) | χ2=0.270 | 0.603 | |||||||||
| 治疗方案[例(使用率,%)] | ||||||||||||||
| 抗生素治疗 | 45(55.6) | 23(44.2) | 22(75.9) | χ2=7.544 | 0.006 | |||||||||
| 中药治疗 | 47(58.0) | 30(57.7) | 17(58.6) | χ2=0.007 | 0.935 | |||||||||
| 激素治疗 | 9(11.1) | 4(7.7) | 5(17.2) | χ2=0.888 | 0.346 | |||||||||
| 激素治疗时间[d,M(Q1,Q3)] | 6.0(4.0,11.0) | 5.0(3.3,18.3) | 7.0(6.0,11.0) | U=12.500 | 0.556 | |||||||||
| 抗病毒治疗 | 10(12.3) | 5(9.6) | 5(17.2) | χ2=0.420 | 0.517 | |||||||||
| 抗病毒治疗时间[d,M(Q1,Q3)] | 7.0(5.5,12.3) | 7.0(5.0,7.0) | 7.0(7.0,14.0) | U=15.500 | 0.548 | |||||||||
| 实验室检测指标 | ||||||||||||||
| 红细胞计数[×1012/L,M(Q1,Q3)] | 4.1(3.7,4.5) | 4.1(3.7,4.4) | 4.2(3.6,4.6) | U=709.500 | 0.852 | |||||||||
| 血红蛋白[g/L,M(Q1,Q3)] | 122.0(106.0,132.0) | 122.0(108.8,131.3) | 123.0(99.0,133.0) | U=723.000 | 0.760 | |||||||||
| 红细胞压积[%,M(Q1,Q3)] | 36.2(32.4,39.2) | 36.3(32.4,38.9) | 35.8(31.9,39.5) | U=721.500 | 0.939 | |||||||||
| 血小板计数[×109/L,M(Q1,Q3)] | 192.5(144.0,287.8) | 192.5(141.0,241.8) | 195.0(157.8,297.3) | U=797.500 | 0.483 | |||||||||
| 淋巴细胞计数[×109/L,M(Q1,Q3)] | 1.0(0.7,1.6) | 1.0(0.8,1.7) | 1.0(0.6,1.4) | U=616.000 | 0.259 | |||||||||
| 白细胞计数[×109/L,M(Q1,Q3)] | 5.3(3.8,7.2) | 4.7(3.7,6.2) | 6.3(4.4,8.4) | U=994.000 | 0.018λ | |||||||||
| 中性粒细胞计数[×109/L, M(Q1,Q3)] | 3.3(2.2,4.7) | 2.8(2.0,3.7) | 3.7(2.9,6.2) | U=1037.500 | 0.005λ | |||||||||
| 中性粒细胞百分比[%,M(Q1,Q3)] | 64.2(52.8,73.9) | 60.7(51.5,70.0) | 71.3(61.9,77.7) | U=1008.500 | 0.012λ | |||||||||
| CD3+CD4+细胞计数[个/μl, M(Q1,Q3)] | 454.7(301.3,638.6) | 454.7(356.9,638.6) | 361.7(247.5,709.2) | U=24.000 | 0.596 | |||||||||
| CD3+CD4+细胞百分比[%, M(Q1,Q3)] | 39.1(33.4,47.7) | 39.1(33.4,46.3) | 41.4(34.3,47.2) | U=30.000 | 1.000 | |||||||||
| CD3+CD8+细胞计数[个/μl, M(Q1,Q3)] | 344.2(239.6,457.3) | 344.2(199.3,501.9) | 320.7(258.0,396.1) | U=31.000 | 1.000 | |||||||||
| CD3+CD8+细胞百分比[%, M(Q1,Q3)] | 24.7(18.2,34.7) | 21.9(18.2,30.5) | 31.5(22.5,39.1) | U=36.000 | 0.596 | |||||||||
| CD4+/CD8+比值[M(Q1,Q3)] | 1.7(1.0,2.7) | 1.7(1.0,2.7) | 1.4(0.9,2.2) | U=26.000 | 0.736 | |||||||||
| CD3+/CD16+CD56+细胞计数[个/μl,M(Q1,Q3)] | 193.8(105.1,393.8) | 213.1(110.9,393.8) | 143.2(104.8,229.6) | U=25.000 | 0.665 | |||||||||
| CD3+/CD16+CD56+细胞百分比[%,M(Q1,Q3)] | 16.6(12.0,24.8) | 16.6(12.0,29.1) | 17.6(13.5,19.7) | U=26.000 | 0.736 | |||||||||
| CD3+CD19+细胞计数[个/μl, M(Q1,Q3)] | 127.7(63.4,214.5) | 127.7(63.4,211.8) | 144.4(69.4,208.9) | U=31.000 | 1.000 | |||||||||
| CD3+CD19+细胞百分比[%, M(Q1,Q3)] | 8.9(6.3,14.5) | 8.9(6.4,14.5) | 9.7(7.0,13.7) | U=30.000 | 1.000 | |||||||||
| CD3+CD45+细胞计数[个/μl, M(Q1,Q3)] | 841.0(662.8,1162.9) | 845.9(682.2,1162.9) | 727.0(629.2,986.2) | U=24.000 | 0.596 | |||||||||
| CD3+CD45+细胞百分比[%, M(Q1,Q3)] | 67.8(63.8,74.6) | 67.6(60.2,73.6) | 73.3(70.2,75.7) | U=41.000 | 0.307 | |||||||||
| C反应蛋白[mg/L,M(Q1,Q3)] | 9.8(5.3,34.9) | 9.0(1.4,25.8) | 21.4(8.2,48.0) | U=967.500 | 0.009λ | |||||||||
| 降钙素原[ng/ml,M(Q1,Q3)] | 0.0(0.0,0.1) | 0.0(0.0,0.1) | 0.1(0.0,0.2) | U=789.000 | 0.089 | |||||||||
| 血红细胞沉降率[mm/1h, M(Q1,Q3)] | 29.0(14.0,49.0) | 23.0(9.0,45.5) | 38.0(25.0,60.5) | U=835.000 | 0.011 | |||||||||
| 谷丙转氨酶[U/L,M(Q1,Q3)] | 14.7(10.2,23.7) | 14.3(10.2,23.3) | 15.0(10.5,23.7) | U=716.500 | 0.908 | |||||||||
| 谷草转氨酶[U/L,M(Q1,Q3)] | 30.0(23.9,38.0) | 31.3(24.0,38.2) | 28.6(22.8,35.5) | U=625.000 | 0.299 | |||||||||
| 总胆红[μmol/L,M(Q1,Q3)] | 10.1(7.5,13.8) | 10.0(7.3,13.5) | 10.1(7.6,17.0) | U=778.000 | 0.614 | |||||||||
| 内生肌酐清除率[ml/min, M(Q1,Q3)] | 81.3(64.0,102.7) | 79.6(63.6,102.7) | 84.8(64.5,101.0) | U=700.000 | 0.566 | |||||||||
| 活化部分凝血活酶时间[s, M(Q1,Q3)] | 28.1(26.1,32.2) | 28.6(26.3,32.5) | 27.9(25.2,29.9) | U=582.500 | 0.178 | |||||||||
| 血浆凝血酶原时间[s,M(Q1,Q3)] | 11.7(10.8,12.8) | 11.7(10.8,12.7) | 11.7(10.9,12.9) | U=756.500 | 0.663 | |||||||||
| 凝血酶时间[s,M(Q1,Q3)] | 17.4(16.3,18.2) | 17.5(16.2,18.3) | 17.2(16.5,17.9) | U=637.000 | 0.430 | |||||||||
| 心肌肌钙蛋白Ⅰ[ng/ml,M(Q1,Q3)] | 0.05(0.02,0.08) | 0.05(0.02,0.08) | 0.06(0.02,0.08) | U=568.000 | 0.642 | |||||||||
| 乳酸脱氢酶[U/L,M(Q1,Q3)] | 171.0(152.5,206.4) | 169.1(149.9,206.8) | 173.0(161.0,205.0) | U=812.500 | 0.564 | |||||||||
| 肌酸激酶[U/L,M(Q1,Q3)] | 56.0(36.0,86.0) | 60.0(40.8,92.0) | 47.0(36.0,66.0) | U=613.000 | 0.165 | |||||||||
| 肌酸激酶同工酶[U/L,M(Q1,Q3)] | 8.6(7.0,11.2) | 8.0(6.2,11.0) | 8.9(8.0,13.3) | U=903.500 | 0.141 | |||||||||
| [1] |
Tamuzi JL, Ayele BT, Shumba CS, et al. Implications of COVID-19 in high burden countries for HIV/TB: A systematic review of evidence. BMC Infect Dis, 2020, 20(1): 744. doi:10.1186/s12879-020-05450-4.
pmid: 33036570 |
| [2] | Tadolini M, Codecasa LR, García-García JM, et al. Active tuberculosis, sequelae and COVID-19 co-infection: first cohort of 49 cases. Eur Respir J, 2020, 56(1): 2001398. doi:10.1183/13993003.01398-2020. |
| [3] |
Sarkar S, Khanna P, Singh AK. Impact of COVID-19 in patients with concurrent co-infections: A systematic review and meta-analyses. J Med Virol, 2021, 93(4): 2385-2395. doi:10.1002/jmv.26740.
pmid: 33331656 |
| [4] | González-Domenech CM, Pérez-Hernández I, Gómez-Ayerbe C, et al. A Pandemic within Other Pandemics. When a Multiple Infection of a Host Occurs: SARS-CoV-2, HIV and Mycobacterium tuberculosis. Viruses, 2021, 13(5): 931. doi:10.3390/v13050931. |
| [5] | Mousquer GT, Peres A, Fiegenbaum M. Pathology of TB/COVID-19 Co-Infection: The phantom menace. Tuberculosis (Edinb), 2021, 126: 102020. doi:10.1016/j.tube.2020.102020. |
| [6] | Wang Q, Guo S, Wei X, et al. Global prevalence, treatment and outcome of tuberculosis and COVID-19 coinfection: a systematic review and meta-analysis (from November 2019 to March 2021). BMJ Open, 2022, 12(6): e059396. doi:10.1136/bmjopen-2021-059396. |
| [7] |
Petrone L, Petruccioli E, Vanini V, et al. Coinfection of tuberculosis and COVID-19 limits the ability to in vitro respond to SARS-CoV-2. Int J Infect Dis, 2021, 113 Suppl 1: S82-S87. doi:10.1016/j.ijid.2021.02.090.
pmid: 33713816 |
| [8] | Sheerin D, Abhimanyu, Peton N, et al. Immunopathogenic overlap between COVID-19 and tuberculosis identified from transcriptomic meta-analysis and human macrophage infection. iScience, 2022, 25(6): 104464. doi:10.1016/j.isci.2022.104464. |
| [9] | 中华人民共和国国家卫生健康委员会办公厅, 中华人民共和国国家中医药管理局综合司.新型冠状病毒感染诊疗方案(试行第十版). 国卫办医急函〔2023〕4号. 2023-01-05. |
| [10] | 中华人民共和国国家卫生和计划生育委员会. WS 288—2017 肺结核诊断. 2017-11-09. |
| [11] | Tiberi S, Utjesanovic N, Galvin J, et al. Drug resistant TB-latest developments in epidemiology, diagnostics and management. Int J Infect Dis, 2022, 124 Suppl 1: S20-S25. doi:10.1016/j.ijid.2022.03.026. |
| [12] |
Hartnady Z, Krehbiel B, Stenzel A, et al. Outcomes and Clinical Characteristics of COVID-19 in Patients with Tuberculosis: A Retrospective Matched Cohort Study. Infect Dis Rep, 2023, 15(2): 204-209. doi:10.3390/idr15020021.
pmid: 37102981 |
| [13] | Udoakang AJ, Djomkam Zune AL, Tapela K, et al. The COVID-19, tuberculosis and HIV/AIDS: Ménage à Trois. Front Immunol, 2023, 14: 1104828. doi:10.3389/fimmu.2023.1104828. |
| [14] | Langford BJ, So M, Raybardhan S, et al. Antibiotic prescribing in patients with COVID-19: rapid review and meta-analysis. Clin Microbiol Infect, 2021, 27(4): 520-531. doi:10.1016/j.cmi.2020.12.018. |
| [15] |
Bonow RO, Fonarow GC, O’Gara PT, et al. Association of Coronavirus Disease 2019 (COVID-19) With Myocardial Injury and Mortality. JAMA Cardiol, 2020, 5(7): 751-753. doi:10.1001/jamacardio.2020.1105.
pmid: 32219362 |
| [16] |
Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet, 2020, 395(10223): 497-506. doi:10.1016/S0140-6736(20)30183-5.
pmid: 31986264 |
| [17] |
Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet, 2020, 395(10229): 1054-1062. doi:10.1016/S0140-6736(20)30566-3.
pmid: 32171076 |
| [18] | Liu K, Fang YY, Deng Y, et al. Clinical characteristics of novel coronavirus cases in tertiary hospitals in Hubei Province. Chin Med J (Engl), 2020, 133(9): 1025-1031. doi:10.1097/CM9.0000000000000744. |
| [19] |
Zheng M, Gao Y, Wang G, et al. Functional exhaustion of antiviral lymphocytes in COVID-19 patients. Cell Mol Immunol, 2020, 17(5): 533-535. doi:10.1038/s41423-020-0402-2.
pmid: 32203188 |
| [20] | Diao B, Wang C, Tan Y, et al. Reduction and Functional Exhaustion of T Cells in Patients With Coronavirus Disease 2019 (COVID-19). Front Immunol, 2020, 11(1): 827. doi:10.3389/fimmu.2020.00827. |
| [21] | Sy KTL, Haw NJL, Uy J. Previous and active tuberculosis increases risk of death and prolongs recovery in patients with COVID-19. Infect Dis (Lond), 2020, 52(12): 902-907. doi:10.1080/23744235.2020.1806353. |
| [1] | Wu Xuan, Zhang Yanqiu, Xu Jiying, Meng Dan, Sun Dingyong. Analysis of factors influencing the treatment outcomes of patients with pulmonary tuberculosis and diabetes mellitus in Henan Province (2019—2023) [J]. Chinese Journal of Antituberculosis, 2025, 47(4): 425-431. |
| [2] | Zhang Guoqin, Qu Ting, Meng Qinglin, Zhou Lin, Liu Eryong. Implementation update of strategy for the control of tuberculosis and HIV/AIDS co-infection in China [J]. Chinese Journal of Antituberculosis, 2025, 47(1): 12-17. |
| [3] | Pan Meimin, Li Wenjuan, Zhang Xuehong, Yang Lihui, He Juan, Tan Yongwei. Study on serum TNFSF14 and sIL-2R levels in elderly patients with pulmonary tuberculosis and their correlation with short-term prognosis [J]. Chinese Journal of Antituberculosis, 2025, 47(1): 66-71. |
| [4] | Fan Jun, Wang Heng, Lan Tinglong, Dong Weijie, Tang Kai, Li Yuan, Yan Guangxuan, Xu Shangsheng, Kang Zhigang, Qin Shibing. Clinical characteristics and surgical outcomes of 12 cases of non-tuberculous mycobacterial spondylitis [J]. Chinese Journal of Antituberculosis, 2025, 47(1): 87-95. |
| [5] | Wang Fei, Hua Duo, Guo Jianjian, Liu Chang, Han Lu, Ren Yi. Characteristic analysis of non-tuberculous mycobacterial pulmonary disease patients in Wuhan area from 2021 to 2023 [J]. Chinese Journal of Antituberculosis, 2024, 46(9): 1069-1076. |
| [6] | Palidanguli Abudureheman, Wang Senlu, Gulina Badeerhan, Wang Le, Zulikatiayi Abudula, Wang Xinqi, Maiwulajiang Yimamu, Wang Xijiang. Distribution of Mycobacterium tuberculosis genotypes in Kashgar region and their association with clinical characteristics of pulmonary tuberculosis patients [J]. Chinese Journal of Antituberculosis, 2024, 46(9): 1077-1082. |
| [7] | Yang Liangzi, Zhang Peize, Lu Shuihua. Interpretation of World Health Organization’s Co-administration of Treatment for Drug-resistant Tuberculosis and Hepatitis C: 2024 Update [J]. Chinese Journal of Antituberculosis, 2024, 46(8): 874-876. |
| [8] | Cai Qinghe, Fu Hui, Chen Ruiming, Fan Youming, Yang Qingwei. Analysis of the clinical characteristics and influencing factors of pulmonary tuberculosis patients with diabetes mellitus in Shantou City from 2016 to 2022 [J]. Chinese Journal of Antituberculosis, 2024, 46(8): 926-934. |
| [9] | Chai Dongyu, Qin Shuyi, Zhang Ronghua, Zou Nannan, Wang Xin. Analysis of risk factors for viral pneumonia combined with invasive pulmonary mycosis [J]. Chinese Journal of Antituberculosis, 2024, 46(7): 750-755. |
| [10] | Fu Keyan, Zhu Bangzheng, Ye Jian. Research progress on interstitial lung disease combined with Mycobacterium tuberculosis infection [J]. Chinese Journal of Antituberculosis, 2024, 46(7): 823-829. |
| [11] | Liu Guizhen, Deng Guofang. Interpretation of Evidence and research gaps identified during development of policy guidelines for tuberculosis (Second edition): tuberculosis related comorbidity [J]. Chinese Journal of Antituberculosis, 2024, 46(6): 618-624. |
| [12] | Yang Rui, Li Ling, Chen Jinou, Xu Lin. Analysis of influencing factors of anti-tuberculosis treatment effect for pulmonary tuberculosis patients complicated with diabetes in Yunnan Province from 2017 to 2021 [J]. Chinese Journal of Antituberculosis, 2024, 46(5): 519-524. |
| [13] | Liu Meijun, Li Feng. Current situation and research progress of co-infection of HIV/AIDS and subclinical tuberculosis [J]. Chinese Journal of Antituberculosis, 2024, 46(5): 596-600. |
| [14] | Yang Jieying, Xiao Xincai, Du Yuhua, Lai Keng, He Liqian, Wang Ting, Lin Ying, He Weiyun. Analysis of epidemiological characteristics and therapeutic prognosis among pulmonary tuberculosis patients complicated with diabetes mellitus in Guangzhou City from 2014 to 2023 [J]. Chinese Journal of Antituberculosis, 2024, 46(12): 1504-1510. |
| [15] | Sun Qingfeng, Li Haoran, Pang Yu, Gao Mengqiu. Co-morbidity research progress of tuberculosis and depression [J]. Chinese Journal of Antituberculosis, 2024, 46(1): 106-111. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||
 京公网安备11010202007215号
Total visitors: Visitors of today: Now online:
京公网安备11010202007215号
Total visitors: Visitors of today: Now online:
 This work is licensed under Creative Commons Attribution 3.0 License.
This work is licensed under Creative Commons Attribution 3.0 License.