
Chinese Journal of Antituberculosis ›› 2018, Vol. 40 ›› Issue (9): 932-939.doi: 10.3969/j.issn.1000-6621.2018.09.005
• Original Articles • Previous Articles Next Articles
Tong-qiang ZHANG1,Lin SUN2,Wei GUO1,Cai-li ZHOU1,Li-xin REN1,Zhuo FU1,Shu-jing LI1,A-dong SHEN2,†( ),Yong-sheng XU1,†()
),Yong-sheng XU1,†()
Received:2018-07-02
Online:2018-09-10
Published:2018-10-17
Contact:
A-dong SHEN,Yong-sheng XU
E-mail:shenad16@hotmail.com;drxu69@gmail.com
Tong-qiang ZHANG,Lin SUN,Wei GUO,Cai-li ZHOU,Li-xin REN,Zhuo FU,Shu-jing LI,A-dong SHEN,Yong-sheng XU. The evaluation of tuberculous meningitis scoring system in the diagnose of tuberculous meningitis in children[J]. Chinese Journal of Antituberculosis, 2018, 40(9): 932-939. doi: 10.3969/j.issn.1000-6621.2018.09.005
Add to citation manager EndNote|Ris|BibTeX
URL: http://www.zgflzz.cn/EN/10.3969/j.issn.1000-6621.2018.09.005
| 分类 | 评分指标 | 得分 |
|---|---|---|
| 临床标准(最高6分) | 症状超过5d | 4 |
| 提示存在结核全身中毒症状(1个及多个):体质量减轻或者不增长;盗汗、持续咳嗽>2周 | 2 | |
| 近1年内有与肺结核患者密切接触史或者TST或(和)IGRA阳性者(仅限于<10岁儿童) | 2 | |
| 神经系统检查有局灶性神经系统缺失症状与体征表现(除外脑神经麻痹) | 1 | |
| 脑神经麻痹 | 1 | |
| 意识改变 | 1 | |
| 脑脊液标准(最高4分) | 清亮 | 1 |
| 白细胞计数(10~500)×106 个/L | 1 | |
| 淋巴细胞比例(>0.50) | 1 | |
| 蛋白浓度>1g/L | 1 | |
| 脑脊液葡萄糖/血葡萄糖浓度<0.5,或脑脊液葡萄糖浓度<2.2mmol/L | 1 | |
| 头颅影像学表现(最高6分) | 脑积水 | 1 |
| 基底脑膜强化 | 2 | |
| 结核瘤 | 2 | |
| 脑梗死 | 1 | |
| 强化前基底部高密度影 | 2 | |
| 其他部位结核感染的证据 | 胸片有活动性肺结核的表现:肺结核=2,粟粒型肺结核=4 | 2/4 |
| (最高4分) | 神经系统外CT/MRI/B型超声检查发现有结核病表现 | 2 |
| 从痰、淋巴结、胃液、尿液、血等培养出MTB或者抗酸杆菌染色阳性 | 4 | |
| 从神经系统外标本中检测到MTB核酸b | 4 |

| TBM评分系统参数 | TBM组 (102例) | 比率 (%) | 病毒性脑炎 组(125例) | 比率 (%) | χ2值 | P值 |
|---|---|---|---|---|---|---|
| 临床标准 | ||||||
| 症状超过5d | 95 | 93.14 | 43 | 34.40 | 81.30 | <0.001 |
| 结核全身中毒症状 | 48 | 47.06 | 2 | 1.60 | 67.58 | <0.001 |
| 结核病接触史 | 21 | 20.59 | 2 | 1.60 | 17.82 | <0.001 |
| TST阳性 | 51 | 50.00 | 1 | 0.80 | 76.99 | <0.001 |
| IGRA | 74 | 72.55 | 1 | 0.80 | 130.79 | <0.001 |
| 神经系统局灶缺失表现 | 11 | 10.78 | 1 | 0.80 | 11.18 | 0.001 |
| 脑神经麻痹 | 24 | 23.53 | 1 | 0.80 | 26.61 | <0.001 |
| 意识改变 | 58 | 56.86 | 30 | 24.00 | 25.55 | <0.001 |
| 脑脊液标准 | ||||||
| 清亮 | 98 | 96.08 | 125 | 100.00 | 4.99 | 0.025 |
| 白细胞数(10~500)×106个/L | 94 | 92.16 | 77 | 61.60 | 28.22 | <0.001 |
| 淋巴细胞比例(>50%) | 90 | 88.24 | 96a | 88.89 | 0.02 | 0.882 |
| 蛋白浓度>1.0g/L | 76 | 74.51 | 0 | 0.00 | 140.01 | <0.001 |
| 脑脊液葡萄糖/血葡萄糖浓度<0.5,或脑脊液葡萄糖浓度<2.2mmol/L | 85 | 83.33 | 2 | 1.60 | 158.74 | <0.001 |
| 脑影像学表现 | ||||||
| 脑积水 | 41 | 40.20 | 1 | 0.80 | 57.81 | <0.001 |
| 基底脑膜强化 | 78 | 76.47 | 7 | 5.60 | 120.44 | <0.001 |
| 结核瘤 | 11 | 10.78 | 0 | 0.00 | 14.17 | <0.001 |
| 脑梗死 | 7 | 6.86 | 0 | 0.00 | 8.85 | 0.003 |
| 强化前基底高密度 | 4 | 3.92 | 0 | 0.00 | 4.99 | 0.025 |
| 肺结核或肺外结核的其他表现 | ||||||
| 肺结核 | 48 | 47.06 | 0 | 0.00 | 74.60 | <0.001 |
| 粟粒型肺结核 | 24 | 23.53 | 0 | 0.00 | 32.89 | <0.001 |
| 神经系统外CT/MR/B型超发现有结核病表现 | 11 | 10.78 | 0 | 0.00 | 11.92 | 0.001 |
| 其他部位标本抗酸杆菌染色阳性或(和)培养出MTB | 15 | 14.71 | 0 | 0.00 | 19.78 | <0.001 |
| 神经系统外标本中检测到MTB核酸 | 21 | 20.59 | 2 | 1.60 | 20.18 | <0.001 |
| 诊断方法 | TBM组(例) | 病毒性脑炎组(例) | 敏感度 (%) | χ2值a | P值a | 特异度 (%) | χ2值b | P值b | ||
|---|---|---|---|---|---|---|---|---|---|---|
| 阳性 | 阴性 | 阳性 | 阴性 | |||||||
| TBM评分系统 | 92 | 10 | 0 | 125 | 90.20 | 100.00 | ||||
| 脑脊液DNA | 14 | 71 | 4 | 106 | 16.47 | 100.64 | <0.001 | 96.36 | 0.67 | 0.415 |
| 脑脊液MTB培养 | 11 | 91 | 0 | 125 | 10.78 | 128.66 | <0.001 | 100.00 | - | - |
| 脑脊液抗酸染色 | 16 | 86 | 2 | 123 | 15.69 | 113.65 | <0.001 | 98.40 | 0.50 | 0.478 |
| TST | 51 | 51 | 1 | 124 | 50.00 | 39.31 | <0.001 | 99.20 | 0.00 | 1.000 |
| IGRA | 74 | 28 | 1 | 124 | 72.55 | 10.48 | 0.001 | 99.20 | 0.00 | 1.000 |
| 基底脑膜强化 | 78 | 24 | 7 | 118 | 76.47 | 6.92 | 0.009 | 94.40 | 5.29 | 0.021 |
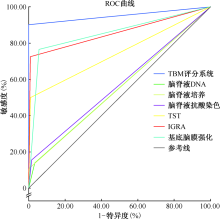
| 诊断方法 | ROC曲线下面积 | Z值a | P值a |
|---|---|---|---|
| TBM评分系统 | 0.951 | ||
| 脑脊液DNA | 0.564 | 9.11 | <0.001 |
| 脑脊液MTB培养 | 0.554 | 9.33 | <0.001 |
| 脑脊液抗酸染色 | 0.570 | 8.96 | <0.001 |
| TST | 0.746 | 5.27 | <0.001 |
| IGRA | 0.859 | 2.81 | 0.005 |
| 基底脑膜强化 | 0.854 | 2.96 | 0.003 |
| [1] |
李淑艳, 凌再芹, 战云飞 , 等. 1992—2011年山东省胸科医院住院儿童结核病患者临床流行病学分析. 中国防痨杂志, 2014,36(10):905-910.
doi: 10.3969/j.issn.1000-6621.2014.10.010 URL |
| [2] |
Marais S, Thwaites G, Schoeman JF , et al. Tuberculous me-ningitis: a uniform case definition for use in clinical research. Lancet Infect Dis, 2010,10(11):803-812.
doi: 10.1016/S1473-3099(10)70138-9 URL pmid: 20822958 |
| [3] | 江载芳, 申昆玲, 沈颖 , 等. 实用儿科学. 8版. 北京: 人民卫生出版社, 2015: 1093-1094. |
| [4] | 陈宗波 . 儿童中枢神经系统病毒性感染的诊断与治疗. 实用儿科临床杂志, 2008,23(10):728-732. |
| [5] |
Wu XR, Yin QQ, Jiao AX , et al. Pediatric tuberculosis at Beijing Children’s Hospital: 2002—2010. Pediatrics, 2012,130(6):e1433-1440.
doi: 10.1542/peds.2011-3742 URL pmid: 23184116 |
| [6] |
van Well GT, Paes BF, Terwee CB , et al. Twenty years of pediatric tuberculous meningitis: a retrospective cohort study in the western cape of South Africa. Pediatrics, 2009,123(1):e1-8.
doi: 10.1542/peds.2008-1353 URL |
| [7] |
van Toorn R, Solomons R . Update on the diagnosis and mana-gement of tuberculous meningitis in children. Semin Pediatr Neurol, 2014,21(1):12-18.
doi: 10.1016/j.spen.2014.01.006 URL pmid: 24655399 |
| [8] |
Zhang YL, Lin S, Shao LY , et al. Validation of thwaites’ diagnostic scoring system for the differential diagnosis of tuberculous meningitis and bacterial meningitis. Jpn J Infect Dis, 2014,67(6):428-431.
doi: 10.7883/yoken.67.428 URL |
| [9] |
Martinez L, Shen Y, Mupere E , et al. Transmission of Mycobacterium tuberculosis in households and the community: A systematic review and meta-analysis. Am J Epidemiol, 2017,185(12):1327-1339.
doi: 10.1093/aje/kwx025 URL |
| [10] |
Hauck FR, Neese BH, Panchal AS , et al. Identification and management of latent tuberculosis infection. Am Fam Physician, 2009,79(10):879-886.
doi: 10.1186/1471-2296-10-34 URL pmid: 19496388 |
| [11] |
Yaramiᶊ A, Gurkan F, Elevli M , et al. Central nervous system tuberculosis in children: a review of 214 cases. Pediatrics, 1998,102(5):e49.
doi: 10.1542/peds.102.5.e49 URL |
| [12] | 毕美华, 熊菀 . 儿童结核性脑膜炎170例临床研究. 重庆医学, 2012,41(31):3273-3275. |
| [13] |
van der Weert EM, Hartgers NM, Schaaf HS , et al. Compari-son of diagnostic criteria of tuberculous meningitis in human immunodeficiency virus-infected and uninfected children. Pediatr Infect Dis J, 2006,25(1):65-69.
doi: 10.1097/01.inf.0000183751.75880.f8 URL |
| [14] |
Andronikou S, Smith B, Hatherhill M , et al. Definitive neuroradiological diagnostic features of tuberculous meningitis in children. Pediatr Radiol, 2004,34(11):876-885.
doi: 10.1007/s00247-004-1237-1 URL pmid: 15378213 |
| [15] | 李雪莲, 高孟秋 . 结核性脑膜炎患者行脑脊液实验室检测方法的现状与进展. 中国防痨杂志, 2018,40(3):320-324. |
| [16] |
Kennedy DH, Fallon RJ . Tuberculous meningitis. JAMA, 1979,241(3):264-268.
doi: 10.1001/jama.1979.03290290032021 URL |
| [17] |
Solomons RS, van Elsland SL, Visser DH , et al. Commercial nucleic acid amplification tests in tuberculous meningitis-a meta-analysis. Diagn Microbiol Infect Dis, 2014,78(4):398-403.
doi: 10.1016/j.diagmicrobio.2014.01.002 URL |
| [18] | Cecchini D, Ambrosioni J, Brezzo C , et al. Tuberculous me-ningitis in HIV-infected and non-infected patients: comparison of cerebrospinal fluid findings. Int J Tuberc Lung Dis, 2009,13(2):269-271. |
| [19] |
Youssef FG, Afifi SA, Azab AM , et al. Differentiation of tuberculous meningitis from acute bacterial meningitis using simple clinical and laboratory parameters. Diagn Microbiol Infect Dis, 2006,55(4):275-278.
doi: 10.1016/j.diagmicrobio.2006.01.027 URL |
| [20] |
Karande S, Gupta V, Kulkarni M , et al. Prognostic clinical variables in childhood tuberculous meningitis: an experience from Mumbai, India. Neurol India, 2005,53(2):191-195.
doi: 10.4103/0028-3886.16407 URL |
| [21] |
Tung YR, Lai MC, Lui CC , et al. Tuberculous meningitis in infancy. Pediatr Neurol, 2002,27(4):262-266.
doi: 10.1016/S0887-8994(02)00431-9 URL |
| [22] | 母发光, 何海兰, 谭泰昌 , 等. γ-干扰素释放试验对儿童结核性脑膜炎的诊断价值. 临床儿科杂志, 2015,33(3):242-246. |
| [23] | Mutsvangwa J, Millington KA, Chaka K , et al. Identifying recent Mycobacterium tuberculosis transmission in the setting of high HIV and TB burden. Thorax, 2010,65(4):312-320. |
| [24] |
Ersoy Y, Yetkin F, Bayraktar MR , et al. A new diagnostic scoring for discrimination of tuberculous and bacterial meningitis on the basis of clinical and laboratory findings. Med Princ Pract, 2012,21(3):259-263.
doi: 10.1159/000333808 URL |
| [25] |
Solomons RS, Wessels M, Visser DH , et al. Uniform research case definition criteria differentiate tuberculous and bacterial meningitis in children. Clin Infect Dis, 2014,59(11):1574-1578.
doi: 10.1093/cid/ciu665 URL |
| [26] |
Solomons RS, Visser DH, Marais BJ , et al. Diagnostic accuracy of a uniform research case definition for TBM in children: a prospective study. Int J Tuberc Lung Dis, 2016,20(7):903-908.
doi: 10.5588/ijtld.15.0509 URL |
| [27] |
Hristea A, Olaru ID . Applying a consensus case definition to patients with confirmed tuberculous meningitis. Int J Infect Dis, 2012,16(10):e758-759.
doi: 10.1016/j.ijid.2012.04.013 URL pmid: 22738790 |
| [1] | LIU Xiao-li, LEI Li-mei, GUO Zhou-li, HUANG Yin, XU Jing, ZHAO Xia, WANG Yan, FU Li. Study on the relationship of stigma and social support of tuberculosis patients [J]. Chinese Journal of Antituberculosis, 2020, 42(9): 1002-1008. |
| [2] | Academic Working Committee of Chinese Antituberculosis Association, Editorial Board of Chinese Journal of Antituberculosis . Expert consensus of clinical application of fixed-dose combination formulations [J]. Chinese Journal of Antituberculosis, 2020, 42(9): 885-893. |
| [3] | JIN Hong-jian. The construction of tuberculosis prevention and control service system at county level in China needs to be strengthened urgently —— Comments and suggestions of an old tuberculosis control and prevention worker [J]. Chinese Journal of Antituberculosis, 2020, 42(9): 896-902. |
| [4] | ZHANG Can-you, XIA Hui, CHENG Jun. Testing and reporting requirements for Class Ⅱ biosafety cabinet in tuberculosis laboratory [J]. Chinese Journal of Antituberculosis, 2020, 42(9): 903-909. |
| [5] | ZHOU Lin, LIU Er-yong, MENG Qing-lin, CHEN Ming-ting, ZHOU Xin-hua, GAO Wei-wei, LIN Ming-gui, XIE Ru-ming. Evaluation of the quality of pulmonary tuberculosis diagnosis after the implementation of the newly revised WS 288-2017 Diagnosis for pulmonary tuberculosis standards [J]. Chinese Journal of Antituberculosis, 2020, 42(9): 910-915. |
| [6] | LIU Er-yong, WANG Qian, ZHOU Lin, ZHANG Guo-qin, ZHANG Xiu-lei, MA Yong-cheng, YANG Shu-min, WANG Cui, MENG Qing-lin, CHEN Ming-ting, LIN Ming-gui, TU De-hua.. Analysis of diagnostic quality of pulmonary tuberculosis with negative etiology in some areas of China [J]. Chinese Journal of Antituberculosis, 2020, 42(9): 916-920. |
| [7] | MENG Qing-lin, LI Jin-lan, LIN Ding-wen, MA Yong-cheng, HOU Shuang-yi, LIU Nian-qiang, ZHOU Lin. Analysis of the awareness about knowledge on the updated TB diagnosis standard among the practitioners in TB control institutions [J]. Chinese Journal of Antituberculosis, 2020, 42(9): 921-925. |
| [8] | WANG Qian, ZHOU Lin, LIU Er-yong, ZHAO Yan-lin, LI Tao, CHEN Ming-ting, YANG Li-jia, WANG Jia.. A survey on the diagnostic ability of tuberculosis in the county-level medical institutions in China [J]. Chinese Journal of Antituberculosis, 2020, 42(9): 926-930. |
| [9] | LI Ting, HE Jin-ge, SU Qian, LI Jing, LI Yun-kui, GAO Wen-feng, GAO Yuan, YANG Wen. Value of tuberculin test in screening tuberculosis infection in HIV infected/AIDS patients in Butuo County, Sichuan Province [J]. Chinese Journal of Antituberculosis, 2020, 42(9): 931-936. |
| [10] | LI Yun-kui, HE Jin-ge, SU Qian, LI Ting, LI Jing, GAO Wen-feng, YANG Wen, MAO Guang-yu. Value of tuberculin test in screening tuberculosis infection in HIV infected/AIDS patients in Butuo County, Sichuan Province [J]. Chinese Journal of Antituberculosis, 2020, 42(9): 937-941. |
| [11] | SU Qian, XIA Yong, LU Jia, WANG Dan-xia, HE Jin-ge. Analysis on the epidemiological characteristics of pulmonary tuberculosis among children aged 0-14 in Sichuan Province from 2009 to 2018 [J]. Chinese Journal of Antituberculosis, 2020, 42(9): 942-947. |
| [12] | DENG Ya-li, ZHANG Tian-hua, LIU Wei-ping, ZHANG Hong-wei, MA Yu, LI Peng.. Temporal and spatial clustering analysis of pulmonary tuberculosis incidence in Shaanxi Province from 2014 to 2018 [J]. Chinese Journal of Antituberculosis, 2020, 42(9): 948-955. |
| [13] | DONG Xiao, ZHAO Zhen, LIU Nian-qiang, WANG Sen-lu, CUI Yan. Analysis of the finding characteristics of pulmonary tuberculosis in the elderly population in Xinjiang Uygur Autonomous Region during 2009—2017 [J]. Chinese Journal of Antituberculosis, 2020, 42(9): 956-961. |
| [14] | LIANG Rui-yun, FANG Wei-jun, REN Hui-li, LI Hui-ru, ZHANG Hui. Study on CT manifestations of non-tuberculous mycobacterium pulmonary disease patients with and without diabetes mellitus [J]. Chinese Journal of Antituberculosis, 2020, 42(9): 962-967. |
| [15] | MA Ting-long, HAN Yi, CHENG Xu, LIU Zhi-dong. Clinical observation on treatment effectiveness of transdermal ultrasound-mediated drug delivery combined with oral anti-tuberculosis drug in patients with chest wall tuberculosis [J]. Chinese Journal of Antituberculosis, 2020, 42(9): 968-972. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||
 京公网安备11010202007215号
Total visitors: Visitors of today: Now online:
京公网安备11010202007215号
Total visitors: Visitors of today: Now online:
 This work is licensed under Creative Commons Attribution 3.0 License.
This work is licensed under Creative Commons Attribution 3.0 License.