| [1] |
MA Yan, LU Wei, GAO Lei, CHU Nai-hui, ZHOU Lin, CHENG Shi-ming.
To end tuberculosis epidemic needs strengthen the management of screening and preventive treatment of latent tuberculosis infection in high-risk groups
[J]. Chinese Journal of Antituberculosis, 2022, 44(3): 209-214.
|
| [2] |
XU Cai-hong, ZHAO Yan-lin.
Build an intelligent network to promote tuberculosis prevention and treatment
[J]. Chinese Journal of Antituberculosis, 2022, 44(3): 215-218.
|
| [3] |
XIE Li, ZHU Hui, GAO Jing-tao, LIU Zhong-quan, MA Li-ping, ZHANG Li-qun, GE Qi-ping, NIE Li-hui, KONG Zhong-shun, WU Xiao-guang, LIU Rong-mei, CHEN Hong-mei, SONG Yan-hua, LI Qiang, LYU Zi-zheng, LIU Yu-hong, LU Yu, PANG Yu, GAO Meng-qiu.
Changes of plasma concentration of bedaquiline during the treatment of drug-resistant pulmonary tuberculosis and its assocation with QTc interval prolongation
[J]. Chinese Journal of Antituberculosis, 2022, 44(3): 219-226.
|
| [4] |
LI Dong-shuo, WANG Bin, LU Yu, XU Jian.
Study of expression and function of Mycobacterium tuberculosis membrane protein MmpL5-MmpS5
[J]. Chinese Journal of Antituberculosis, 2022, 44(3): 227-233.
|
| [5] |
ZHANG Yu-xia, XIONG Yu, CHANG Ting-ting, LIU Feng-xia.
Analysis of adverse reactions of bedaquiline containing regimen in the treatment of drug-resistant pulmonary tuberculosis
[J]. Chinese Journal of Antituberculosis, 2022, 44(3): 239-245.
|
| [6] |
QI Qi, CAI Qing-shan, CUI Yan-fei, CHEN Yuan-yuan, BAO Zhi-jian, QIU Mei-hua, GUO Yi-nan, MA Xiao-qing.
Effect of Roast Radix Glycyrrhizae Decoction Granules on the prolongation of QT interval caused by bedaquiline in the treatment of multidrug-resistant pulmonary tuberculosis
[J]. Chinese Journal of Antituberculosis, 2022, 44(3): 246-251.
|
| [7] |
YUE Ying, HUANG Ting-ting, REN Fei, MA Jin-bao, QI Yun.
Congenital drug-resistant tuberculosis: a case report and literature review
[J]. Chinese Journal of Antituberculosis, 2022, 44(3): 252-257.
|
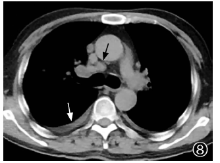
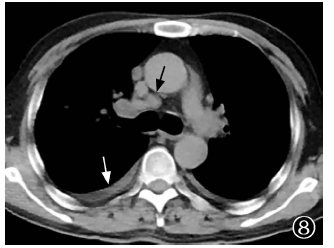
| [8] |
LI Duo, LYU Yan, LYU Ping-xin.
Study of MRI characteristics of spinal tuberculous meningitis and the change after anti-tuberculosis treatment
[J]. Chinese Journal of Antituberculosis, 2022, 44(3): 258-263.
|
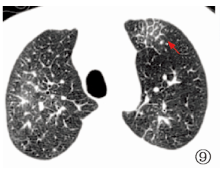
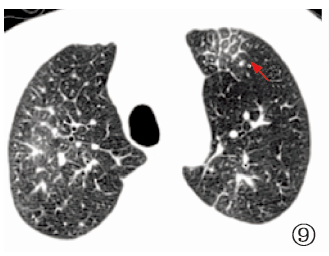
| [9] |
CHEN Meng-meng, DONG Jing, SUN Qi, HUANG Mai-ling, DING Ze-yu, SHI Yu-ting, JIA Hong-yan, DU Bo-ping, WEI Rong-rong, XING Ai-ying, ZHANG Zong-de, PAN Li-ping.
Diagnostic performance of differentially expressed miRNA identified by gene chip in discriminating tuberculous meningitis from viral meningitis
[J]. Chinese Journal of Antituberculosis, 2022, 44(3): 264-272.
|
| [10] |
ZHUANG Li, MA Zi-feng, JIANG Yu-wei, HUANG Xing, ZHANG Hui-yong, LU Zhen-hui, WU Xian-wei.
Mechanism of traditional Chinese medicine “Qinbudan” in the treatment of pulmonary tuberculosis based on network pharmacology
[J]. Chinese Journal of Antituberculosis, 2022, 44(3): 273-283.
|
| [11] |
ZHANG Li-juan, ZHANG Hua, WANG Xia-fang, SHI Mei-hua, FENG Yan-jun, ZHANG Jian-ping, TANG Pei-jun.
The value of the ratio of tuberculosis specific antigen to CD4+ T cell count in the auxiliary diagnosis of AIDS complicated with pulmonary tuberculosis
[J]. Chinese Journal of Antituberculosis, 2022, 44(3): 284-288.
|
| [12] |
FAN Ru, LI Xiao-fei.
Research progress of molecular biology detection technology for tuberculosis
[J]. Chinese Journal of Antituberculosis, 2022, 44(3): 294-298.
|
| [13] |
ZHANG Hui, ZHAO Yan-lin.
Strengthen multi-sectoral cooperation mechanism to further promote the tuberculosis prevention and control in China
[J]. Chinese Journal of Antituberculosis, 2022, 44(2): 115-119.
|
| [14] |
SUN Zhao-gang.
Attention should be paid to the research and development of Mycobacterium tuberculosis antigen detection technology
[J]. Chinese Journal of Antituberculosis, 2022, 44(2): 120-124.
|
| [15] |
LIU Li-qin, XU Zu-hui, HUANG Yi-sheng, YAO Qi-neng, TAN Yun-hong, ZHOU Lin, XIA Yin-yin, LIU Er-yong, HUANG Guo-jun, BAI Li-qiong, CHENG Shi-ming.
Study on the clinical efficacy of a 4-month treatment program for the initial treatment of smear-negative pulmonary tuberculosis with Mycobacterium vaccae Vaccine immune intervention
[J]. Chinese Journal of Antituberculosis, 2022, 44(2): 125-130.
|

 ), LEI Mei2, QIN Li-xin3
), LEI Mei2, QIN Li-xin3
 京公网安备11010202007215号
Total visitors: Visitors of today: Now online:
京公网安备11010202007215号
Total visitors: Visitors of today: Now online:
 This work is licensed under Creative Commons Attribution 3.0 License.
This work is licensed under Creative Commons Attribution 3.0 License.