Email Alert | RSS 帮助

中国防痨杂志 ›› 2022, Vol. 44 ›› Issue (3): 289-293.doi: 10.19982/j.issn.1000-6621.20210561
杨澄清1, 梅春林1, 杜荣辉1( ), 雷美2, 秦立新3
), 雷美2, 秦立新3
YANG Cheng-qing1, MEI Chun-lin1, DU Rong-hui1(), LEI Mei2, QIN Li-xin3
摘要:
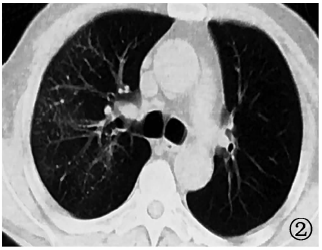
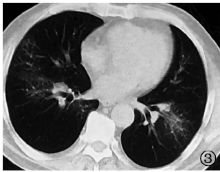
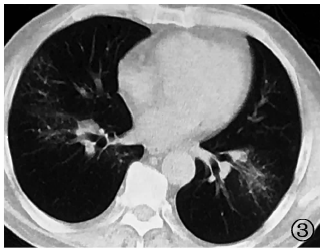
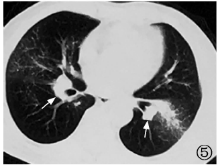
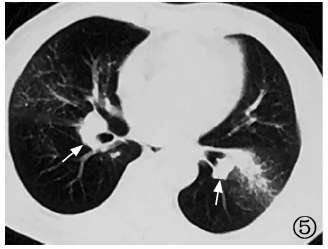
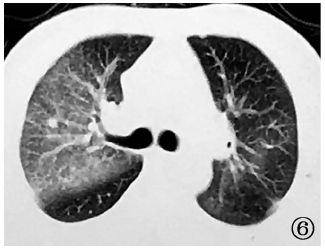
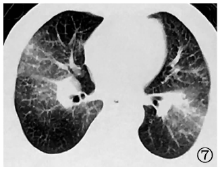
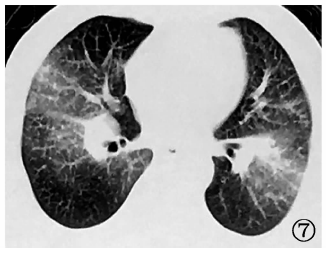
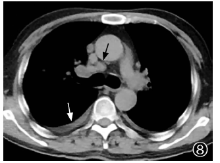
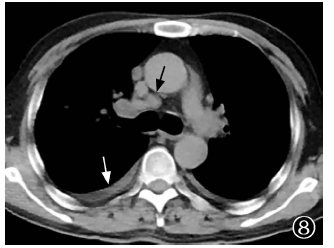
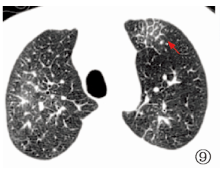
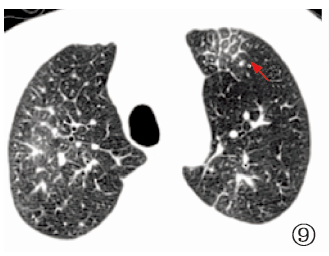
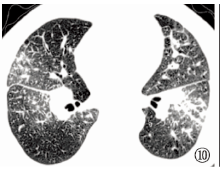
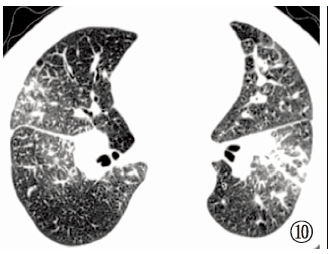
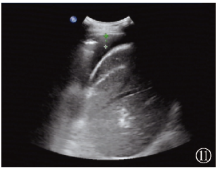
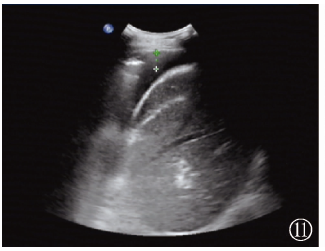
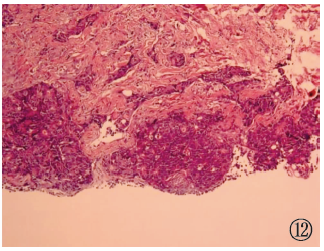
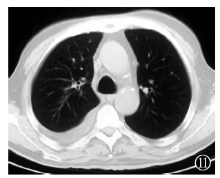
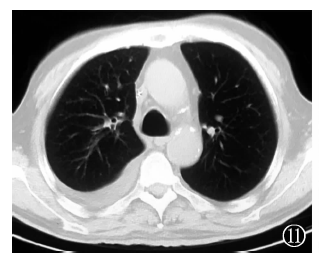
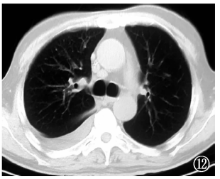
2019年4月17日,武汉市肺科医院呼吸科收治1例69岁男性因外院结核分子生物学阳性诊断为肺结核的肺癌性淋巴管炎患者。该患者因“发现肺部阴影3个月,间断咳嗽2个月”入院。既往有结肠癌病史。胸部CT扫描显示双肺弥漫性沿支气管血管束分布结节伴磨玻璃影,伴小叶间隔增厚,双肺门及纵隔淋巴结肿大,双侧胸腔积液,在外院行肺泡灌洗液(BALF)GeneXpert MTB/RIF(简称“ GeneXpert”)检出MTB(极低)及TB-PCR检出MTB,诊断为肺结核,转诊至武汉市肺科医院。入院后完善结核相关检查,PPD皮肤试验阴性,γ干扰素释放试验阴性,胸部CT影像学特征不符合肺结核改变,临床怀疑BALF结核病病原分子生物学检测假阳性,建议患者复查BALF、GeneXpert及经气管镜超声引导针吸活检术(EBUS-TBNA),患者拒绝。给予诊断性胸腔穿刺,抽出胸腔积液20ml,送检显示,癌胚抗原(118.4μg/L)明显升高,提示恶性胸腔积液;最后行内科胸腔镜胸膜活检,提示转移性低分化腺癌,结合胸部CT表现,诊断为肺癌性淋巴管炎。患者后因病情恶化死亡。笔者认为,影像学表现为沿支气管血管束分布结节伴小叶间隔增厚及纵隔淋巴结肿大时需鉴别肺癌性淋巴管炎。影像学表现与肺结核不相符时,分子生物学阳性诊断肺结核需谨慎,以避免误诊误治。
中图分类号:
 京公网安备11010202007215号
ip访问总数: ip当日访问总数: 当前在线人数:
京公网安备11010202007215号
ip访问总数: ip当日访问总数: 当前在线人数:
 本作品遵循Creative Commons Attribution 3.0 License授权许可
本作品遵循Creative Commons Attribution 3.0 License授权许可