Email Alert | RSS 帮助

中国防痨杂志 ›› 2020, Vol. 42 ›› Issue (4): 360-365.doi: 10.3969/j.issn.1000-6621.2020.04.011
张兴,王凤鸣,吕旭峰,华天齐,张学军,蒋靖怡,丁陈丽,朱伟,夏国栋,吉俊敏( ),赵飞()
),赵飞()
ZHANG Xing,WANG Feng-ming,LYU Xu-feng,HUA Tian-qi,ZHANG Xue-jun,JIANG Jing-yi,DING Chen-li,ZHU Wei,XIA Guo-dong,JI Jun-min(),ZHAO Fei()
摘要:
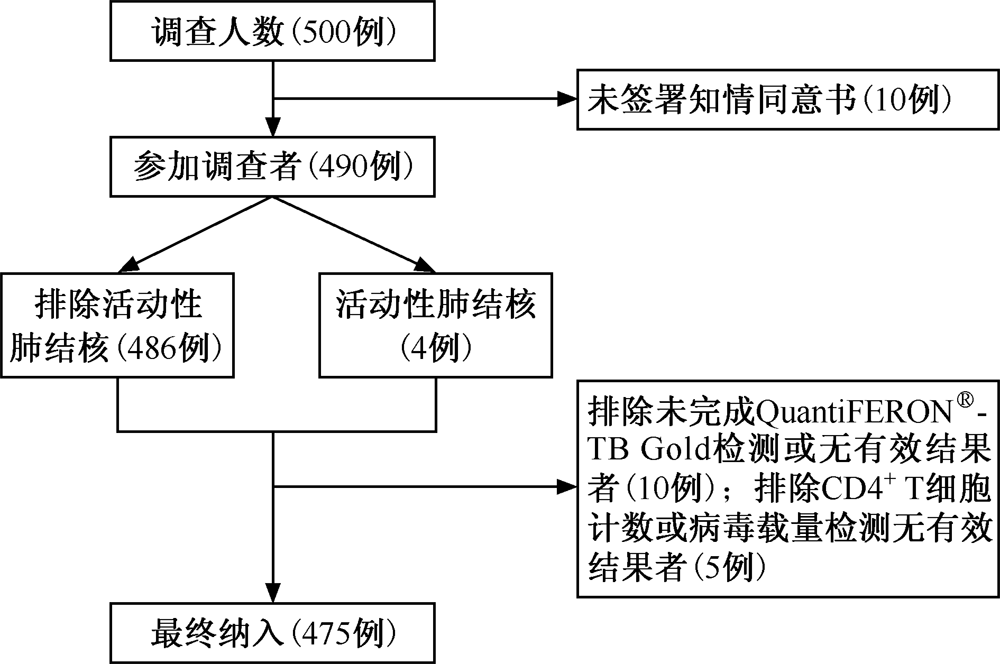
目的 分析HIV感染/AIDS者结核感染情况及其影响因素。方法 于2017年1—7月采用随机整群抽样的方法,抽取江苏省常州地区3家社区医院,以其10年累计登记的HIV感染/AIDS者作为研究对象,最终纳入475例,平均年龄(44.44±13.85)岁,其中,男378例(79.58%),女97例(20.42%);HIV感染者273例(57.47%),AIDS患者202例(42.53%)。收集研究对象的社会人口学信息及临床相关信息;采集研究对象外周静脉血,检测HIV病毒载量,并选取CD4 +T细胞计数>200个/μl者采用QuantiFERON ®-TB Gold (QFT)检测结核感染情况;分析研究对象结核感染情况,并采用多因素非条件logistic回归分析结核感染的影响因素。结果 研究对象中CD4 +T细胞计数>200个/μl者有429例,结核感染率为10.02%(43/429)。单因素分析显示,CD4 +T细胞计数>200个/μl者中有结核病接触史者结核感染率(30.30%,10/33)高于无接触史者(8.33%,33/396);CD4 +T细胞计数>500个/μl者结核感染率(13.15%,33/251)高于CD4 +T细胞计数为200~500个/μl者(5.62%,10/178),差异均有统计学意义(χ 2分别为16.30、6.55,P值均<0.05)。进一步的非条件logistic回归分析显示,CD4 +T细胞计数>200个/μl的HIV感染/AIDS者中,有结核病患者接触史者结核感染风险是无接触史者的4.61倍[调整OR值(95%CI值)为4.61(2.00~10.63)];CD4 +T细胞计数>500个/μl的HIV感染/AIDS者结核感染风险是CD4 +T细胞计数200~500个/μl者的2.47倍[调整OR值(95%CI值)为2.47(1.17~5.21)]。结论 免疫水平低下的HIV感染/AIDS者结核感染检出率低;结核病患者接触史、免疫水平是HIV感染/AIDS者结核感染的重要影响因素。
 京公网安备11010202007215号
ip访问总数: ip当日访问总数: 当前在线人数:
京公网安备11010202007215号
ip访问总数: ip当日访问总数: 当前在线人数:
 本作品遵循Creative Commons Attribution 3.0 License授权许可
本作品遵循Creative Commons Attribution 3.0 License授权许可