Email Alert | RSS 帮助

中国防痨杂志 ›› 2021, Vol. 43 ›› Issue (8): 832-837.doi: 10.3969/j.issn.1000-6621.2021.08.015
陈珊珊, 唐晓军, 唐小莉, 戴广川, 曾谊( ), 张侠()
), 张侠()
CHEN Shan-shan, TANG Xiao-jun, TANG Xiao-li, DAI Guang-chuan, ZENG Yi(), ZHANG Xia()
摘要:
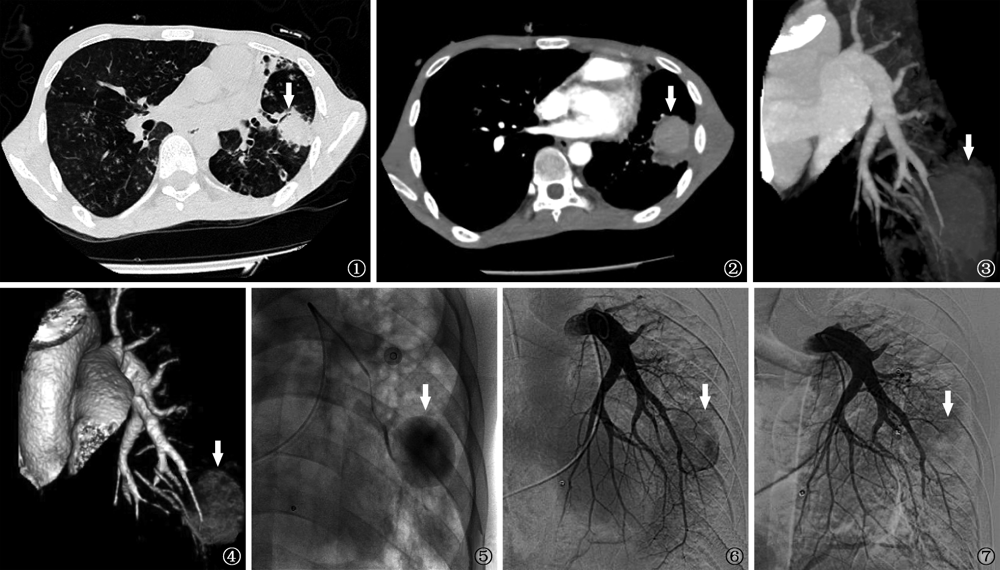
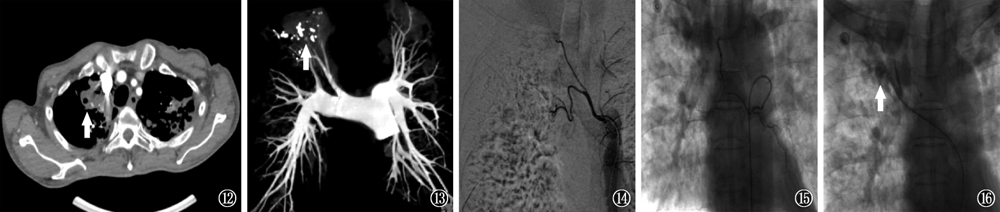
目的 总结和分析动脉栓塞介入治疗肺结核相关肺动脉假性动脉瘤(pulmonary artery pseudoaneurysms,PAP)伴大咯血的临床特征。方法 对南京市第二医院行动脉介入栓塞治疗的3例肺结核并发PAP伴大咯血患者的临床表现、治疗及预后进行报道。并以“pulmonary tuberculosis”和“pulmonary artery pseudoaneurysms”或“Rasmussen’s aneurysm”为检索词检索PubMed数据库,检索时间为2011年1月至2020年12月,剔除综述类文献、重复发表及资料不全等文献,纳入肺结核并发PAP患者临床资料完整的文章,收集患者的临床特征、影像学表现、PAP分型、诊治方法及预后,并进行文献复习。结果 病例1~3均确诊为肺结核并发大咯血,影像学提示肺结核空洞性病灶,且经胸部CT血管造影(CTA)及肺动脉造影均发现PAP继发于结核空洞壁上的肺动脉血管。其中,病例1,男,24岁,以“痰中带血7d,加重3d(咯血量>500ml/d,意识不清)”为主要表现,行支气管动脉栓塞术后再次大咯血,再行左胸廓内动脉和左胸外侧动脉、左侧肺动脉栓塞术后咯血停止;病例2,女,65岁,以“咯血5d(100ml/次,2次/d)伴胸闷”为主要表现,行支气管动脉栓塞术后再次大咯血,再行右侧肺动脉栓塞术后咯血停止;病例3,男,58岁,以“咳嗽、胸闷、盗汗4个月,咯血3d(300ml)”为主要表现,行双侧支气管动脉栓塞术后仍有咯血,再行左右支气管动脉、右上肺动脉栓塞术后咯血停止。通过筛选共获得21篇文献,42例肺结核并发PAP患者,与本文3例患者共计45例,其中男性36例,女9例,中位年龄为52.0(35.0,63.0)岁。45例患者均进行了CTA,PAP的检出率为100.0%;41例进行了肺动脉造影,PAP的检出率为75.6%(31例)。41例患者接受了血管介入治疗,其中26例行肺动脉栓塞治疗,7例行支气管动脉栓塞治疗,8例接受了支气管动脉栓塞+肺动脉栓塞治疗,术后有效止血40例,1例患者因大咯血窒息死亡。术后40例获得随访,2例复发,分别经外科切除术和再次行支气管动脉栓塞而治愈。结论 PAP是导致肺结核大咯血的主要原因之一,肺动脉介入栓塞治疗仍是PAP并发大咯血的首选干预措施。当支气管动脉栓塞效果不佳或咯血近期复发时,应及时进行胸部CTA检查,以排除PAP可能。
 京公网安备11010202007215号
ip访问总数: ip当日访问总数: 当前在线人数:
京公网安备11010202007215号
ip访问总数: ip当日访问总数: 当前在线人数:
 本作品遵循Creative Commons Attribution 3.0 License授权许可
本作品遵循Creative Commons Attribution 3.0 License授权许可