Email Alert | RSS 帮助

中国防痨杂志 ›› 2020, Vol. 42 ›› Issue (4): 391-397.doi: 10.3969/j.issn.1000-6621.2020.04.017
范欣欣,吴迪,林友飞,陈晓红( )
)
FAN Xin-xin,WU Di,LIN You-fei,CHEN Xiao-hong()
摘要:
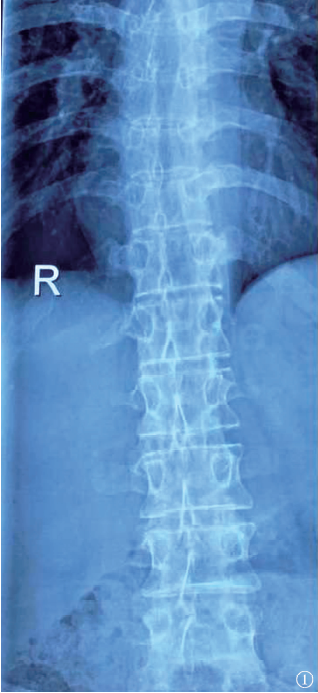
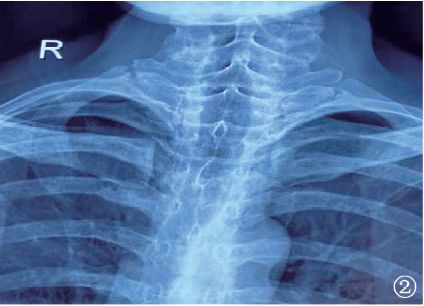
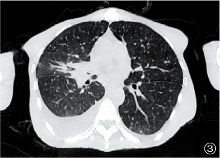
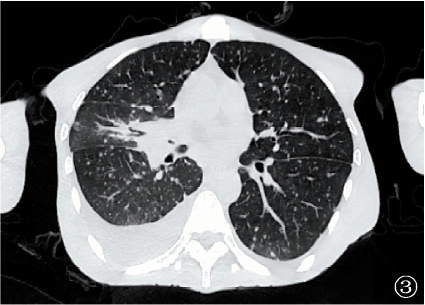
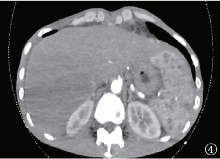
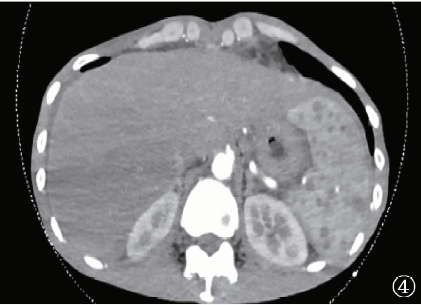
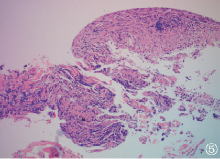
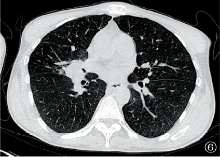
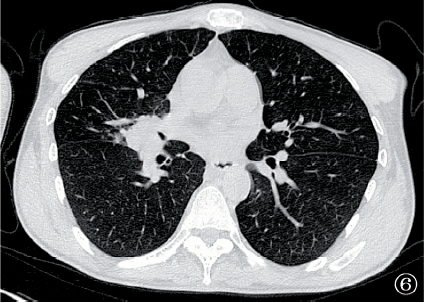
目的 探讨应用阿达木单克隆抗体(简称“单抗”)治疗强直性脊柱炎致播散性结核病的临床特点、诊治要点和治疗转归。 方法 回顾性分析福建省福州肺科医院2019年6月10日收治的1例应用阿达木单抗治疗强直性脊柱炎致播散性结核病的临床资料、诊治经过及随访情况,并进行文献复习。以“adalimumab”和“disseminated tuberculosis”为检索词对PubMed数据库进行检索,以“阿达木单抗”和“播散性结核病”为检索词通过万方数据库和中国知网对中文文献进行检索,检索时间截止到2019年9月,经过筛选剔除,共获取相关文献34篇,其中中文文献0篇,英文文献34篇。删去重复的文献并剔除可能为阿达木单抗以外的肿瘤坏死因子α(TNF-α)致播散性结核病及TNF-α致其他播散性疾病的报道,共筛选出具备详细病例资料的文献8篇,共获得8例患者,结合本研究收集的患者,对其临床特征、诊断和治疗情况进行分析。 结果 本例患者为男性,28岁。因“强直性脊柱炎”接受阿达木单抗治疗,治疗2个月后出现咳嗽、气促、腹胀、发热,入院后经胸部CT、胸膜活检及支气管镜等检查,诊断为“播散性结核病(双肺、右侧支气管、胸腔、腹腔、心包、纵隔淋巴结、锁骨上淋巴结、腹腔淋巴结、盆腔淋巴结、脾)”。给予“3H-R-Z-E/9H-R-E”方案治疗,辅以异烟肼支气管局部雾化吸入,行抗结核药物治疗后症状改善。治疗第5个月,CT复查提示“肺部病变减少,纵隔内部分淋巴结肿大较前缩小,增厚的支气管管壁较前变薄,管腔较前通畅,胸、腹腔积液明显吸收。截止到2019年12月,患者仍处于规则的抗结核药物治疗中。文献检索后获得8例患者,加上本例,共9例患者。其中,男3例,女6例;年龄9~75岁,平均年龄(50.44±25.19)岁。9例患者中,5例开始使用阿达木单抗治疗之前的结核病筛查试验结果为阴性,1例既往有抗结核治疗史,1例曾进行过预防性抗结核治疗,3例有与结核病患者的密切接触史。诊断明确行抗结核药物治疗后,5例患者转归良好。3例转归差,其中1例病情持续进展,并发消化道出血;1例颅内病灶持续进展;1例出现急性呼吸窘迫综合征,最终死亡。1例转归不明。 结论 阿达木单抗可致播散性结核病,准备接受阿达木单抗治疗的患者均应在用药前进行结核病筛查,治疗过程中应该警惕潜伏性结核感染转为活动性结核病及新发结核感染,停用阿达木单抗和及时行抗结核药物治疗是预后良好的关键。
 京公网安备11010202007215号
ip访问总数: ip当日访问总数: 当前在线人数:
京公网安备11010202007215号
ip访问总数: ip当日访问总数: 当前在线人数:
 本作品遵循Creative Commons Attribution 3.0 License授权许可
本作品遵循Creative Commons Attribution 3.0 License授权许可