Email Alert | RSS 帮助

中国防痨杂志 ›› 2022, Vol. 44 ›› Issue (6): 576-581.doi: 10.19982/j.issn.1000-6621.20210648
刘鑫, 郭乐, 李军孝, 陈其亮, 仵倩红( )
)
LIU Xin, GUO Le, LI Jun-xiao, CHEN Qi-liang, WU Qian-hong()
摘要:
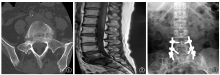
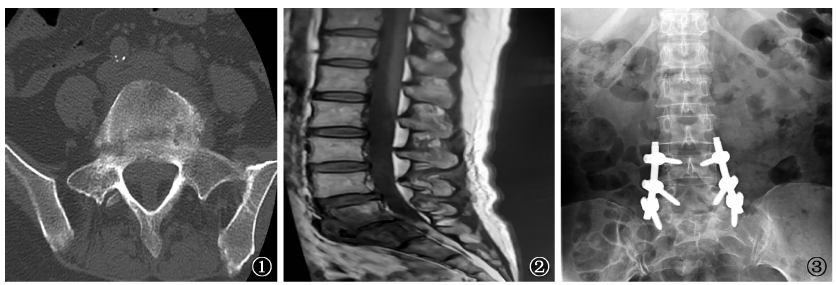
目的: 对误诊为腰椎结核的布鲁氏菌性脊柱炎患者进行分析,探讨布鲁氏菌性脊柱炎的治疗结局。 方法: 收集陕西省结核病防治院2018年6月至2021年6月误诊为腰椎结核的6例布鲁氏菌性脊柱炎患者的临床资料,对临床症状、实验室检查结果、影像学表现、治疗方法及随访结果进行分析。 结果: 6例患者中,男性4例,女性2例;年龄54~81岁,平均(63.00±10.15)岁;2例有布鲁氏菌病接触史,3例有牧区及牛羊接触史,1例接触史不详;1例合并陈旧性肺结核,1例硬膜外脓肿患者行手术治疗。病程20d至1年,平均(4.17±1.32)个月;误诊时间7~24d,平均(15.66±5.53)d;病变部位位于腰2~3椎体2例,腰3~4椎体1例,腰4~5椎体2例,腰5~骶1椎体并发硬膜外脓肿1例。6例患者X线检查均表现为椎间隙狭窄,椎体为边缘型骨质破坏且与增生硬化交替出现,邻近椎间骨桥形成;1例高热,体温>39℃,为波状热,其余5例体温正常;2例结核菌素纯蛋白衍生物(PPD)皮肤试验弱阳性,3例一般阳性,3例结核抗体阳性,2例结核蛋白芯片(LAM抗体)及结核感染T细胞斑点试验(T-SPOT.TB)阳性。所有患者通过虎红平板凝集试验初筛及试管凝集试验阳性确诊为布鲁氏菌性脊柱炎,经盐酸多西环素、利福平治疗12周,随访6个月,最终4例治愈,2例好转,未见复发。 结论: 布鲁氏菌性脊柱炎一般有疾病接触史,通过热型及实验室检查可确诊,布鲁氏菌性脊柱炎患者总体预后良好。
 京公网安备11010202007215号
ip访问总数: ip当日访问总数: 当前在线人数:
京公网安备11010202007215号
ip访问总数: ip当日访问总数: 当前在线人数:
 本作品遵循Creative Commons Attribution 3.0 License授权许可
本作品遵循Creative Commons Attribution 3.0 License授权许可